Skin, Hair and Nails
Acne
Overview: What is Acne?
The information in this section has been gathered from existing peer-reviewed and other literature and has been reviewed by expert dermatologists on the CSPA Medical Advisory Board.
Acne occurs when dead skin cells block the openings of oil and hair follicles, called pores, and trap oil that is naturally produced by the body, called sebum (pronounced see-bum). This leads to increased growth of bacteria within the pores and inflammation. The combination of trapped skin cells and sebum can lead to the formation of whiteheads and blackheads, while the inflammation leads to pimples and cysts on the face, back, scalp, shoulders, arms and/or chest.
Acne is a very common skin disorder and is the one most often seen by doctors in skin patients. Although not life-threatening, acne can cause temporary or sometimes permanent marks on the skin, which can affect a person’s self-esteem and quality of life.
 Acne example
Acne example  Acne Example 2
Acne Example 2  Acne Example 3
Acne Example 3  Acne Example 4
Acne Example 4
While there is no way to accurately predict who will develop acne, you are more likely to experience a severe form of it if one of your parents did, or if you suffer from certain diseases or particular hormonal abnormalities (such as polycystic ovary syndrome or Cushing’s syndrome).
What causes acne?
Acne is linked to the hormone testosterone, which occurs naturally in both sexes. One of the many effects of increased testosterone levels is to stimulate the skin’s oil glands to produce sebum, an oily substance that helps to moisturize the skin. The oil glands lie in the skin’s middle layer, wrapped around hair shafts. Where the shaft extends up to the skin’s surface, this tubular structure is called a follicle.
Overactive oil glands pump large amounts of sebum upward through ducts along the hair shaft to the skin’s surface, where it fills up the follicle and overflows onto the skin. At the same time, the dead skin cells lining the follicle are not shed properly and clog up the follicle. That’s when blackheads and whiteheads begin to appear. Blackheads develop when the blockage is incomplete and air oxidizes the oil, leading to a darkened residue. When the follicle is completely blocked, no air comes into contact with the oil, which then maintains its pale white appearance.
Clogged follicles set up ideal conditions for a common resident follicle bacteria, Propionibacterium acnes (P. acnes), to multiply rapidly inside the follicle, leading to the next stage of acne—what most people call pimples, or “zits.” Various substances released by the P. acnes bacteria provoke local inflammation in the follicle, causing redness, swelling and sometimes tenderness. Doctors call these red bumps papules. When the centres of the papules have a large build-up of inflammatory cells and pus, these blemishes are called pustules. Sometimes, the follicle wall will burst, leading to larger and deeper areas of inflammation, called nodules. The body’s immune system response is to enclose these materials in fluid-filled sacs, called cysts. Both nodules and cysts can be quite painful and can lead to scarring if left untreated.
Symptoms
Acne can be mild, moderate or severe, and its symptoms depend on its severity.
Mild acne (non-inflammatory acne): Most people with mild, or non-inflammatory, acne develop whiteheads and blackheads on their face. Whiteheads are white bumps on the skin made up of collections of trapped sebum and dead skin cells. Blackheads are pin-sized black dots on the skin that form when pores are partially blocked and air oxidizes trapped sebum, creating a dark residue.
Moderate to severe acne (inflammatory acne): Inflammatory acne is more severe and can lead to permanent skin discoloration and scarring. This type of acne causes red bumps to appear on the skin, called pimples, which form when blocked pores become infected with bacteria.
Sometimes pimples burst under the skin and release bacteria into surrounding tissue, creating papules. When inflammation and pus build up in papules, they become pustules, which can feel sore and develop a white pus pocket in their centre.
If the inner walls of the infected pores burst and cause inflammation deeper under the skin, nodules form. The body’s immune system response is to enclose these nodules in fluid-filled sacs, called cysts. Nodules and cysts can be very painful.
Treatment
There are many ways to manage and treat acne. While mild acne may be easy to control with proper skin care and over-the-counter remedies, you will need to see a doctor to treat moderate or severe acne. Generally, treating acne begins with good skin care and progresses to prescriptions or medications as needed.

You want to call your doctor if:
- your acne does not improve after 6 to 8 weeks or it gets worse
- your acne leaves scars
- your pimples become large and hard or filled with fluid
- you develop other symptoms, such as excess facial hair if you are a woman
- your acne began when you started a new medication
Regardless of the treatment chosen, treating acne takes time. Mild acne may clear up in a matter of weeks, but moderate to severe acne may take months or years before the skin clears up.
The idea behind any acne treatment is to stop new blemishes from forming and to help the skin heal, thereby reducing the risk of scarring. The treatment you use will be determined by how well your acne responds. Begin with simple cleansers. If there is no visible improvement in three to four weeks, try a non-prescription topical treatment with benzoyl peroxide or with an antibiotic.
If there is no improvement after six to eight weeks, it’s time to discuss other treatment options with your doctor, such as prescription-strength benzoyl peroxide, antibiotics, retinoids, or combination products. It is important to remember that all acne treatments are meant to control the condition, not cure it.
Generally, you should seek medical help if your acne is severe or is getting worse, if your self-care measures and over-the-counter medicines haven’t helped after several months, or if you are developing scars as your acne does clear up.
Managing Acne
Lifestyle changes, such as choosing the right skin products, are a common first step to controlling acne and usually take 6 to 8 weeks to show any effect.
 Skin type: Most people can use just about any soap, cleanser or gel without worrying too much about how they might affect their skin. That’s because their skin type is “normal,” reflecting the average in terms of moisture content, oil production, surface acidity and chemical sensitivity.
Skin type: Most people can use just about any soap, cleanser or gel without worrying too much about how they might affect their skin. That’s because their skin type is “normal,” reflecting the average in terms of moisture content, oil production, surface acidity and chemical sensitivity.
People with oily skin should look for products that are easy to rinse off, such as most bar soaps and cleansers, so that excess oil goes down the drain. Many of the cleansers intended for acne-prone skin can also help people with oily skin.
People with dry skin should look for water-soluble cleansers that remove makeup and excess oil only. Cleansing sheets that leave a trace of an emollient to recondition dry skin can also help.
People with sensitive skin should avoid cleansers and soaps with fragrances and preservatives. Also, it’s best to avoid scrubs, such as cleansing grains, brushes and loofahs, which can irritate sensitive skin and worsen acne if used too vigorously.
Over-washing: On its own, washing your skin won’t cure or prevent acne, and scrubbing with harsh cleansers or over-washing could end up irritating your skin. But washing twice a day with a mild cleanser and water will certainly help remove excess oil from your skin, which is a step in the right direction.

Cosmetics: Oil-based cosmetics can irritate pores, causing them to swell and become blocked and set up ideal conditions for acne to develop. If you have acne, look for water-based moisturizers and make-up, and apply them lightly. When applying conditioners, gels and sprays to your hair, shield your face to avoid getting any on your skin. (Since these products are designed to coat your hair, they will do the same to your skin and block your pores!) Remember, these products can also transfer from your hair to your pillow and then onto your skin. To avoid this problem, wash your pillowcases frequently and consider wearing your hair off your face while you sleep. There are also flesh-toned, medicated acne lotions that can safely hide acne blemishes. Light powder over an oil-free foundation can provide good cover-up. Be sure to remove cosmetics every night with mild soap or cleansers and water before you sleep.
Non-prescription Treatments
Topical Treatments
Cleansers: Cleansers remove oil, sweat, dirt and make-up from the skin’s surface. For best results, use a water-based, unscented cleanser that is strong enough to remove cosmetics but gentle enough to wash away only excess skin oil.
Medicated treatments: Like cleansers, these treatments remove oil, sweat, dirt and make-up from the skin’s surface, which then clears the way for their active ingredients to be better absorbed by the skin. Make sure to use these medicated cleansers as directed on the label, usually once or twice a day. Overuse can lead to dry, irritated skin.
Apply topical treatments to the entire area where you have acne, not just the visible blemishes since you also want to treat smaller areas before they become worse. Expect to use these treatments for six to eight weeks before you see any substantial improvement. Some topicals contain salicylic acid, which breaks down blackheads; others have as their active ingredient non-prescription strength benzoyl peroxide, which has anti-bacterial effects and also goes to work on blackheads; still, others have only anti-bacterial effects.
Prescription Treatments
 Acne medications available by prescription use a variety of approaches to clear the skin. They may fight inflammation, loosen skin cells, block sebum production, change the body’s hormone balance, or prevent scarring. Many topical treatments are available as both individual and combination formulations (a preparation that contains more than one type of medication). If you have a very severe case of acne where topical therapies and over-the-counter skin care products are not enough, or if you have widespread acne over many body areas, your doctor may prescribe a medication that comes as a pill or even as an injection.
Acne medications available by prescription use a variety of approaches to clear the skin. They may fight inflammation, loosen skin cells, block sebum production, change the body’s hormone balance, or prevent scarring. Many topical treatments are available as both individual and combination formulations (a preparation that contains more than one type of medication). If you have a very severe case of acne where topical therapies and over-the-counter skin care products are not enough, or if you have widespread acne over many body areas, your doctor may prescribe a medication that comes as a pill or even as an injection.
Topical treatments
Benzoyl peroxide: Benzoyl peroxide comes in many different strengths and preparations, including gels, creams, lotions, soaps and even facial masks. It destroys acne-causing bacteria and dissolves the keratin in blackheads, thus unblocking the oil-gland pores. Prescription-strength topical treatments have a concentration of approximately 10 per cent benzoyl peroxide, compared with 2.5 per cent in non-prescription preparations. Some combination topical therapies also contain benzoyl peroxide, typically pairing it with an antibiotic. These products can irritate your skin and, rarely, can cause skin allergies. The peroxide in these products will also bleach the colour from clothing and linens.
Corticosteroids: Corticosteroids are synthetic versions of a hormone made in the body. When applied to the skin, they reduce inflammation, making them useful treatments for inflammatory acne. These medications are applied to acne lesions once or twice daily. If corticosteroids are used for an extended period of time over a large area of skin, the drug may be absorbed into the body, which can cause hormonal problems in rare cases. For this reason, it’s important to follow your doctor’s instructions if you are using a corticosteroid cream or lotion. Don’t bandage, cover or wrap the treated area unless directed by your doctor. Side effects include burning, itching, irritation and dryness.
Dimethicone: Dimethicone is a silicone-based gel that can help prevent scarring caused by severe acne. When applied to skin areas where severe acne is healing, it dries to form a thin, water-tight film that keeps the skin below from drying out while it repairs itself. This helps prevent the formation of scars and the itching, discomfort and discoloration that often accompany them. The gel is massaged into the scarred area twice daily. In rare cases, it can cause skin redness, pain or irritation.
Retinoids: The current standard for treating stubborn acne, retinoids are synthetic by-products of vitamin A that correct the abnormal shedding of the skin cells lining hair follicles. Retinoids also reduce the amount of oil produced by the sebaceous glands, as well as thin the oil so that it can no longer clog pores. It is available by prescription, and your doctor has a number of retinoids in cream and gel form to choose from, including tretinoin, adapalene and tazarotene. Retinoids can be a source of skin irritation if used too often or if the dose is too strong. Here are some general guidelines for using topical retinoids:
- Begin your course of treatment by using the retinoid every other night to see how your skin will react. If your skin doesn’t become irritated after several applications, you can increase to every day, if so directed by your doctor.
- Wait 30 minutes after washing before applying the cream or gel.
- Apply a pea-sized amount to your finger for each affected facial region: forehead, nose/chin and each cheek.
- Apply it gently to the whole region, not just the pimples (don’t simply spot treat). If you apply the medication to the visible pimples only, it won’t prevent new ones from appearing elsewhere.
- Avoid getting any in your eyes, and wash your hands well.
- Don’t layer topical retinoids with any other skin treatment or moisturizer.
- Reduce use if your skin becomes irritated.
Dermatologists recommend that topical retinoids not be used during pregnancy or during nursing because of uncertain risks to the baby. Topical retinoids may also increase sun sensitivity. Discuss with your doctor what kind of sunscreen you should use when outdoors.
Topical acne antibiotics: For mild to medium acne, doctors often prescribe clindamycin, erythromycin or sulfacetamide to destroy the bacteria that cause pimples, boils and cysts. These antibiotic preparations are most often used twice a day to treat whiteheads and small blemishes.
Combination products: These products, which usually combine benzoyl peroxide or a retinoid with an antibiotic, contain two medications to treat acne and help maintain clear skin. Combination products your doctor may prescribe include:
- Topical tretinoin plus erythromycin: Apply once daily before bed after washing your face and patting it dry.
- Topical tretinoin plus clindamycin: Apply once daily before bed after washing your face and patting it dry.
- Topical benzoyl peroxide plus erythromycin: Apply a thin layer once or twice daily after washing your face and patting it dry. This product must be refrigerated. It may bleach clothing and linens.
- Topical benzoyl peroxide plus clindamycin: Apply a thin layer once daily after washing your face and patting it dry. It may bleach clothing and linens.
- Topical benzoyl peroxide plus adapalene: Apply a thin layer once daily after washing your face and patting it dry. It may bleach clothing and linens.
Systemic treatments
Antibiotics: This medication is reserved for people whose acne isn’t responding to topical treatment or who have widespread acne on many areas of the body. Their main effects are to destroy bacteria and reduce inflammation. Mild nausea and indigestion are common side effects, but these tend to ease after a few days. Each antibiotic has its own safety profile and things to do or to avoid for best results; you should discuss them with your doctor. Make sure to follow the prescription instructions and take all your medication (even if your skin clears up before the prescription is finished). The most commonly prescribed antibiotics for acne include:
- tetracycline
- minocycline
- doxycycline
- erythromycin
- trimethoprim
- azithromycin
Oral isotretinoin: The most potent acne medication that doctors prescribe, isotretinoin is usually reserved for severe nodular cystic acne that doesn’t improve with other types of treatment. Virtually everyone responds favourably after one course of oral isotretinoin (usually four to six months), and the benefits last a long time for most patients. If improvement is slow, however, multiple courses may be needed to achieve clear skin.
If you have very oily skin, large blackheads, acne on your chest and back, and if you’re in your early teens, your acne may return after a course of oral isotretinoin. Adult women are also at higher risk of seeing their acne return. Side effects include irritated skin and dry eyes and nasal passages. Just about everybody who takes oral isotretinoin develops dry lips and will need to moisturize several times a day to avoid cracking. Other reported side effects include mood changes, a rise in cholesterol levels, liver problems, joint inflammation and a reduced ability to produce white blood cells. Most side effects become more frequent and more severe with higher doses, and most will disappear within two weeks after reducing the dose or stopping the medication. Periodic blood tests can monitor for cholesterol and changes in how well the liver is working.
Oral isotretinoin can cause birth defects. Women of child-bearing age who use this medication must follow the Pregnancy Prevention Program, which requires the use of two forms of birth control to avoid any possibility of pregnancy one month before the course begins, throughout the whole time the oral isotretinoin is taken, and for one month after stopping the medication. Monthly pregnancy tests are also recommended.
Despite these potential hazards, oral isotretinoin remains the most effective therapy currently available for treating serious, stubborn, cystic acne and for reducing the risk of scarring. Dermatologists tend to be the chief prescriber of oral isotretinoin since it requires accurate dosage, close monitoring and periodic blood tests for best results.
Oral contraceptives: Oral contraceptives can be used by women as a primary treatment for acne or if a woman with acne needs birth control. These pills combine progestin and estrogen, so they alter the hormone balance in the body and reduce testosterone levels. This treatment can improve hormone-based acne breakouts and reduce pore blockages. When used alone, oral contraceptives can be used as a long-term acne therapy for mild to moderate acne breakouts. They can also be used in conjunction with other medications for women with more severe acne. Common side effects associated with long-term use can include nausea, weight gain, breast tenderness, menstrual spotting, and mood swings. More serious side effects, which are less common, include blood clots, stroke, headaches, gallstones, increased blood pressure, and depression.
For women with acne that appears after adolescence, new oral contraceptives combine estrogen with a type of progestogen that is an antiandrogen (i.e., it reduces the testosterone in the body). These can be used in combination with topical and other systemic medications and sometimes can be used after retinoid therapy has concluded in adult-onset acne.
Other Treatments
Corticosteroids: Corticosteroid medications are synthetic versions of a hormone naturally produced by the body. They change the body’s immune response, reducing inflammation in the skin and elsewhere. Your dermatologist may inject severely inflamed acne cysts with a corticosteroid to reduce inflammation, promote healing, and prevent scarring. If used for a long period of time, corticosteroids can cause changes in the body’s hormone production. If your doctor is considering using systemic corticosteroids to treat your acne, he or she will carefully plan the dosing and the duration of treatment to avoid this. A reported side effect is weight gain.
Laser and light therapies: Optical treatments, including intense pulsed light (IPL), pulsed dye lasers (PDL), potassium titanyl phosphate laser (KTP), infrared diode lasers, and broad-spectrum continuous-wave visible light sources (blue-light and blue-red light), have been suggested to reduce acne through heating of glands in the skin and inactivation of acne-causing bacteria. Laser and light therapies treatments are applied on top of the skin. While there is evidence for the short-term benefits of laser and light therapies, longer-term studies still need to be done. Common side effects include skin redness and hyperpigmentation (darker patches on the skin).
Tea tree oil: This is an oil valued for its antimicrobial properties. Tea tree oil is available over the counter and applied on affected skin areas. It should not be taken orally, as it is toxic if swallowed. Although it has been used to treat acne, there is little scientific data to support its use. One trial has suggested that 5 per cent tea tree oil gel reduced both inflammatory and non-inflammatory acne lesions. A common side effect is mild skin irritation.
New medications and treatments for acne may be tested through clinical trials across Canada. To learn more about possible new treatments, visit our clinical trials page [link to CSPA clinical trials page].
Footnotes:
*All information on medical treatments on this site is provided as an overview only. For a complete and up-to-date list of side effects, warnings and precautions, read the product’s package insert and consult your doctor or a pharmacist.
**If you are considering an alternative or complementary therapy, discuss it with your doctor first, and always be sure to keep your doctor up to date about any vitamins, supplements, or other forms of alternative treatment you are taking. Like any medication, alternative therapies can interact with other medications/treatments and, in some cases, have side effects of their own. Remember that “natural” does not necessarily mean “safe.”
Coping and Support
Because our image of ourselves is often tied to how we look, having acne can have lasting psychological effects.  People with moderate to severe acne, particularly if it has led to scarring, may have decreased self-confidence and self-esteem issues, which can lead to social withdrawal and, in some cases, even depression. If you are experiencing negative emotions associated with your acne, consult your doctor. Finding the right treatment and support can make a big difference.
People with moderate to severe acne, particularly if it has led to scarring, may have decreased self-confidence and self-esteem issues, which can lead to social withdrawal and, in some cases, even depression. If you are experiencing negative emotions associated with your acne, consult your doctor. Finding the right treatment and support can make a big difference.
Resources
If you are living with Acne or know someone who is, you may want to stay up-to-date on the condition as well as current treatments and news.
Our Affiliate Member
![]() Acne and Rosacea Society of Canada
Acne and Rosacea Society of Canada
Affiliate Infographic - click her to find out more about the Acne and Rosacea Society of Canada.
Other Resources:
Acne and Rosacea Society of Canada - offering and help - printable pdf
Acne Support Group in Cyberspace [http://asgic.proboards.com/index.cgi].
Acne Patient Decision Aid
This decision aid has six steps to guide you through the process of choosing which treatment option best suits you: https://www.informed-decisions.org/acnepda.php
Alopecia
Overview: What is alopecia?
The information in this section has been gathered from existing peer-reviewed and other literature and has been reviewed by expert dermatologists on the CSPA Medical Advisory Board.
Alopecia is the medical term for hair loss, which can occur in small, isolated areas or over a person’s entire body. It can be temporary or permanent, and tends to occur more often in men than women.
Normal hair loss is a natural consequence of hair growth. Each hair grows for several years and then goes into a resting phase that lasts for several months. After this resting phase, the hair falls out and a new hair starts to grow. We normally lose about 100 hairs a day, although more hair may be lost from excessive brushing, washing or rubbing.
Alopecia has many causes, including an inherited disorder, skin burns, traction (e.g., from hairstyles that pull the hair tightly or compulsive hair pulling), radiation therapy and infections. Some alopecia due to traction may be prevented by loosening hair from tight ponytails or braids.
In some situations, temporary hair loss may occur for other reasons. For example, many people experience more hair loss than normal after major surgery or a severe illness with a high fever. Certain medications, including many cancer treatments, may also cause hair to fall out. Hormonal imbalances, an over- or under-active thyroid, and certain fungal infections can also be the cause. However, when these situations are corrected, the hair usually returns.
In contrast, most cases of alopecia are caused by an underlying disease or genetic predisposition and cannot be prevented. There are many different types of alopecia, but the two most common are adrogenetic alopecia and alopecia areata.
 Alopecia Areata
Alopecia Areata 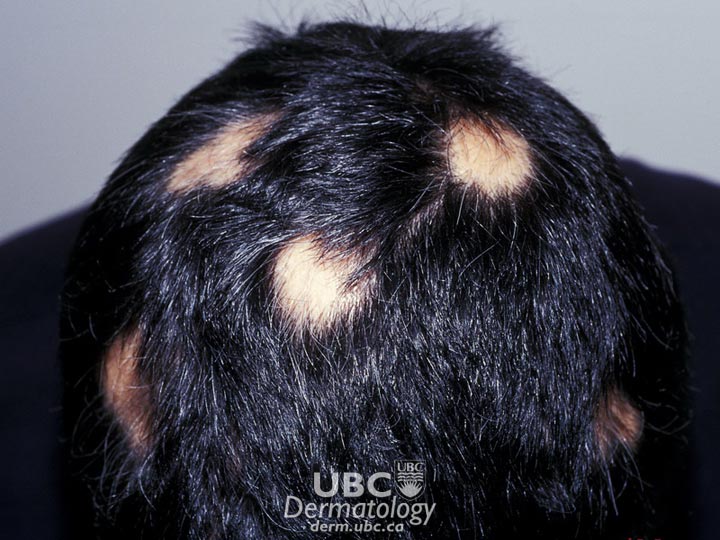 Alopecia Areata 2
Alopecia Areata 2 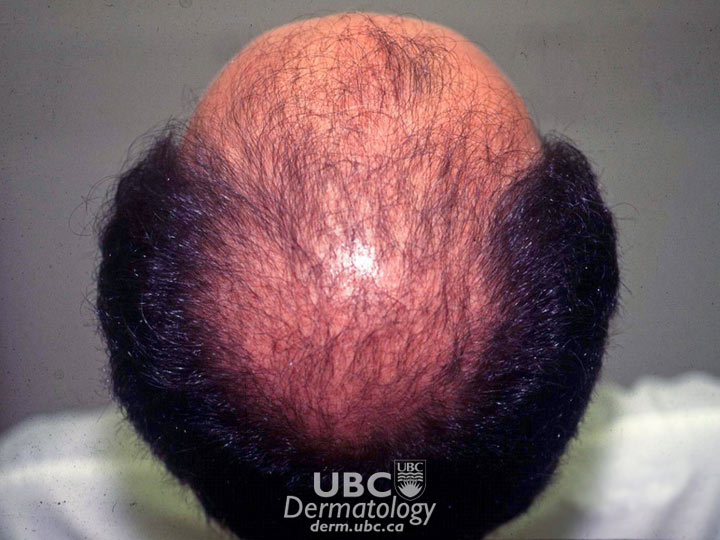 Androgenetic Alopecia
Androgenetic Alopecia
Causes
Androgenetic alopecia (pattern baldness): Androgenetic alopecia can occur in both men and women. In men, androgenetic alopecia is caused by hormonal changes in genetically predisposed individuals. Natural processes in the body convert testosterone, a hormone present in high levels after puberty, to dihydrotestosterone (DHT). DHT acts on hair follicles to slow down or stop hair production, resulting in thinning hair. In women, androgenetic alopecia is also caused by a combination of heredity and hormone levels. However, the mechanism is not currently well understood by scientists. Some research suggests that while even trace levels of testosterone-derived DHT may trigger hair loss in women, other mechanisms may play a role.
Alopecia areata: Alopecia areata is an autoimmune disease that causes groups of hair follicles to be mistakenly attacked by a person’s own immune system. In affected areas, the hairs stop growing and the follicles become very small. Hair production drastically slows, and hair may not appear above the skin’s surface for months or even years. While new research has identified the genes that are linked to this condition, the exact triggers that cause a person’s immune system to attack groups of hair follicles are not known. Research suggests that the triggers may be environmental, stress-related, or viral. The condition is also sometimes associated with other diseases, such as autoimmune thyroid disorders, discoid lupus and secondary syphillis.
Symptoms
In all forms of alopecia, hair loss is frequently the only symptom, but tingling or itching may also be felt in the affected areas.
Androgenetic alopecia

In men, a characteristic pattern of hair loss is most common. Beginning at the temples and/or top of head (toward the back), hair gradually disappears. If these two areas meet the result is complete, or almost complete, baldness.
In both cases, hair loss is permanent, though appropriate treatment may trigger hair follicles to resume hair production.
Alopecia areata
One or more small, round, bare patches on the head and/or elsewhere on the body is common. At the margin of bare patches, broken hairs, wider at the top than at the base, resembling exclamation points appear. No scarring is present. Hair follicles are not permanently damaged and remain capable of producing hair.
In most cases, hair will spontaneously regress, with hair reappearing in a year. However, people who develop the condition before adolescence, are losing hair around the edge of the scalp, have a family history of alopecia areata, or have hay fever, eczema or asthma may be more likely to suffer chronic or permanent hair loss.
In some cases, the nails of the hands or feet may be rough or stippled.
Treatment

Only a physician can confirm the presence of alopecia, so if you experience any of its symptoms, make anappointment to see your doctor. Your doctor will examine your scalp, hair shafts and pattern of hair loss to narrow down potential causes. Determining the cause of the condition is sometimes difficult, so a doctor may take a scalp biopsy, s alp scraping, or blood test to make a diagnosis. A biopsy will help your doctor determine if the hair follicles are healthy and normal, and in the case of alopecia areata, ensure that it is not a symptom of another illness.
Treatment for alopecia varies based on the specific type.
Androgenetic alopecia
There are two medications approved in Canada to treat androgenetic alopecia: minoxidil and finasteride. Both drugs are approved for use by men only.
Minoxidil is a topical solution of 2 per cent minoxidil, applied to the scalp, that effectively promotes hair growth in men and women. A 5 per cent solution is also available. The treatment is continued indefinitely. Discontinuation of treatment results in reversion to hair loss. Side effects include itching and skin irritation.
Finasteride is an oral treatment that effectively promotes hair growth in men. Discontinuation of treatment results in reversion to hair loss. Finasteride is not used to treat the condition in premenopausal women as the drug can affect developing fetuses. In post-menopausal women, finasteride had no effect on hair regrowth. Side effects include loss of sex drive and difficulty achieving an erection.
Other options to treat androgenetic alopecia include hair follicle transplantation and use of cosmetic aids (wigs or hair-weaving techniques).
Alopecia areata
In most cases, alopecia areata will spontaneously regress, with hair reappearing within a year. Because of this, many patients opt for no treatment at all and wear hairpieces, hair weaves or wigs until the hair grows back in. However, in other cases, the disease may persist for long periods or spread to other areas. In approximately 10 per cent of cases, the hair may never regrow. Patients whose alopecia areata began before adolescence or involves the peripheral scalp (ophiasis) or who also have hay fever, eczema or asthma may be at greater risk for progression to the chronic form.
Currently, there are no approved treatments specifically for the disease. However, many agents commonly used to treat other forms of baldness can promote hair growth, though no treatment has been shown to work consistently for all cases. The regrown hair often falls out when treatment is discontinued. However, some ways to treat alopecia areata include:
Corticosteroids
- For small bald patches, corticosteroids may be applied directly to the skin.
- For small and medium-sized areas, corticosteriods are typically injected under the skin in and around the bare patches.
- For larger bare patches, corticosteroids are sometimes given orally. However, hair often falls out when treatment is discontinued. This option is not often used, as some patients may suffer adverse side effects.
Sensitization therapy
Chemicals called contact sensitizers are applied to the area to induce a mild allergic reaction that may trigger hair growth. Common topical contact sensitizers are anthralin, diphenylcyclopropenone (DPCP), dinitrochlorobenzene and squaric acid dibutylester. The use of this treatment is limited to those for whom other treatments are ineffective.
Topical minoxidil
Minoxidil, typically used for male pattern baldness, may be applied to the bare areas. It is not effective in treating those with 100 per cent scalp hair loss.
Psoralen
Psoralen is a compound that enhances absorption of ultraviolet rays. It is usually applied to the skin and followed by exposure to ultraviolet A radiation. This treatment may prevent the immune system from attacking hair follicles. The required frequent exposure to UV light may pose an unacceptable risk of skin cancer. Side effects include skin redness and a burning sensation.
Scientists continue to research alopecia, specifically in the areas of genetics (to determine who is susceptible and why), autoimmunity (to determine the cause and possible treatments) and new medications.
Non-medical treatments
As alopecia areata is often temporary (hair grows back without treatment), some people choose to not treat the condition at all. Many wear a natural-looking wig, hair piece, or hair weave. Other people may consider having a hair transplant. However, a hair transplant involves moving a patient’s own hair follicles from the back or sides of the head to the affected area. For this treatment to work, the person must have healthy hair follicles in these areas. Before deciding which treatment is best for you, talk to your doctor to discuss your expectations as well as each treatment’s limitations. No one treatment is the best for every patient.
*All information on medical treatments on this site is provided as an overview only. For a complete and up-to-date list of side effects, warnings and precautions, read the product’s package insert and consult your doctor or a pharmacist.
**If you are considering an alternative or complementary therapy, discuss it with your doctor first, and always be sure to keep your doctor up to date about any vitamins, supplements, or other forms of alternative treatment you are taking. Like any medication, alternative therapies can interact with other medications/treatments and, in some cases, have side effects of their own. Remember that “natural” does not mean “safe.”
Coping and Support
Alopecia does not negatively impact a person’s overall health. However, a person with the condition may feel emotionally stressed. Some people with alopecia may feel less attractive, especially when their hair loss is extensive. They may also experience frustration, loss, fear, embarrassment, hopelessness or guilt. For these reasons, support from family and friends, as well as professionals (psychiatrists, psychologists, or social workers) can help a person develop a more positive self-image and increased self-confidence.
If your feelings are extreme, or if you find you cannot participate in or enjoy your normal activities (e.g., missing school or work), counselling can be effective. Your family doctor or dermatologist can refer you to professional care.
Not all people with alopecia are affected emotionally. Many men with androgenetic alopecia accept the condition as a natural consequence of aging. And some men and women with alopecia areata take their baldness in stride knowing that, in most cases, their hair will likely grow back on its own. For many patients, the only disruption is the effort that goes into treatment, whether medication-related or not. That being said, support is available for those who seek it.
Resources
Many people with alopecia—whether they seek treatment or not—may want to stay up-to-date on the condition as well as current treatments and news. The following websites are valuable sources of information:
Our Affiliates
 Canadian Alopecia Areata Foundation
Canadian Alopecia Areata Foundation
Other Resources
Atopic Dermatitis (Eczema)
Overview: What is atopic dermatitis?
The information in this section has been gathered from existing peer-reviewed and other literature and has been reviewed by expert dermatologists on the CSPA Medical Advisory Board.
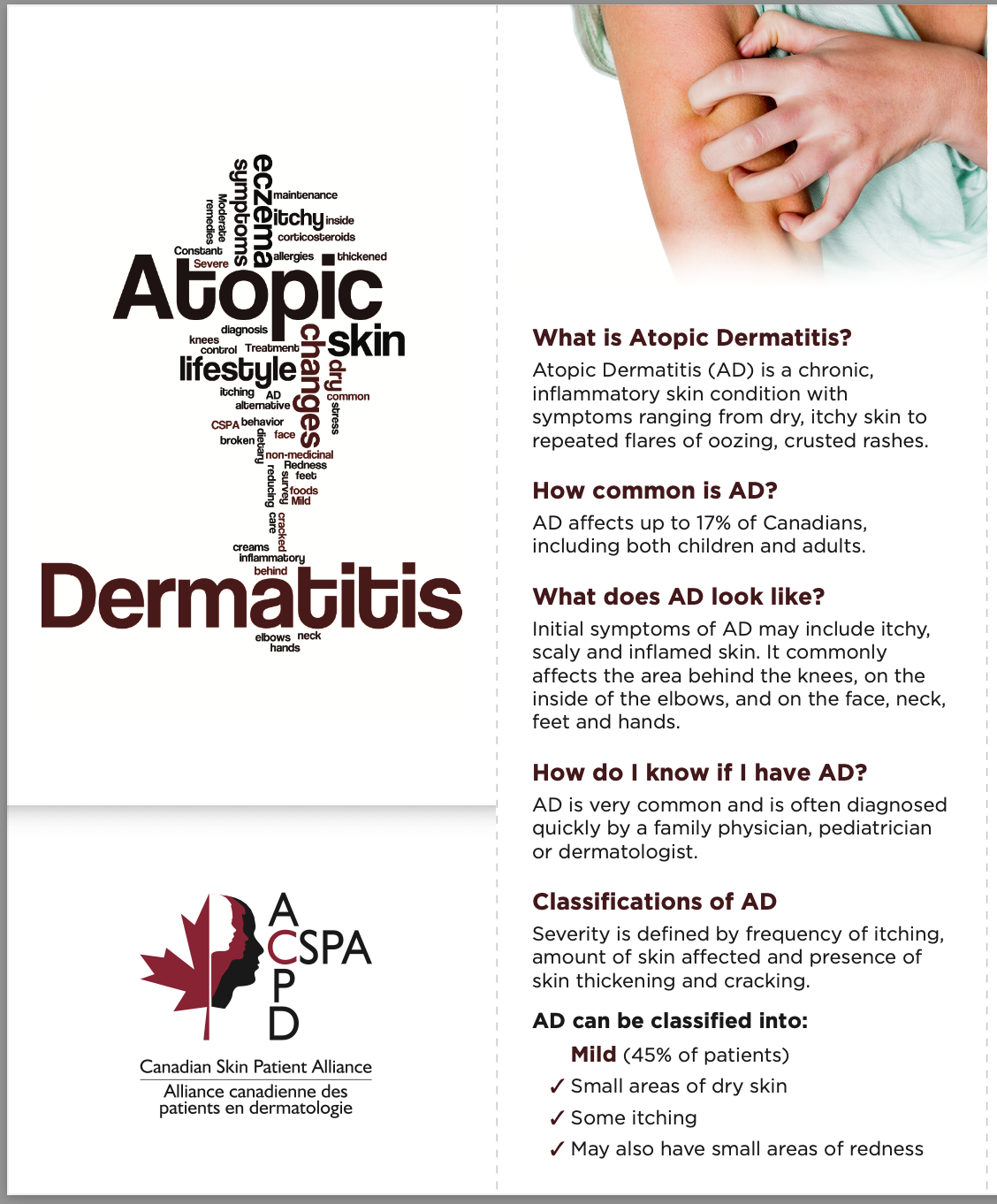
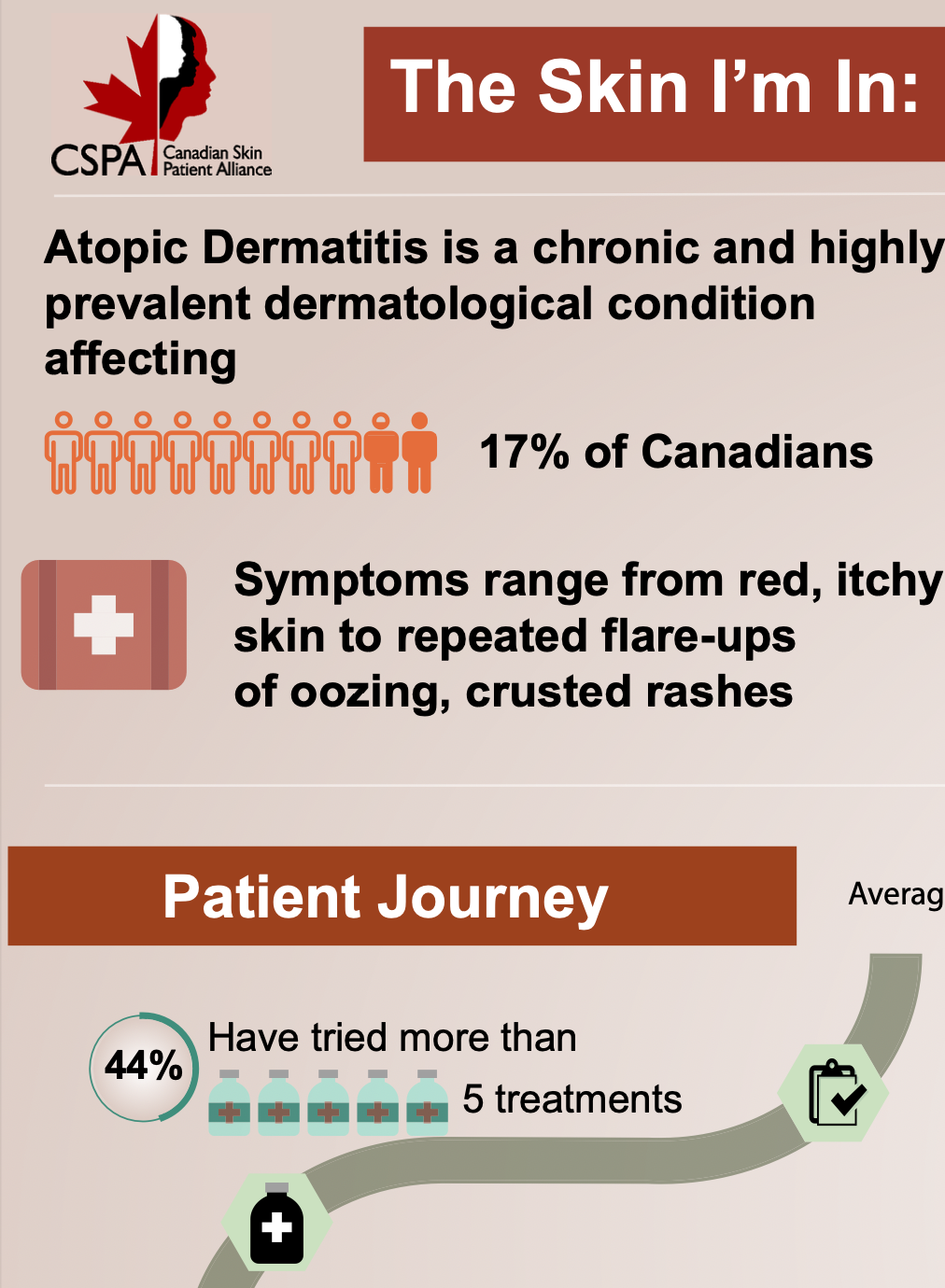
Atopic Dermatitis, also called Eczema, is a term used to describe a group of persistent or chronic conditions that cause inflammation of the upper layers of the skin. It is usually itchy.
Atopic Dermatitis is activated by the immune system and, despite its sometimes unsightly appearance, is not contagious—but it can flare up repeatedly over the course of someone’s life due to triggers such as illness, stress and exposure to allergens and skin irritants. There are four common types of Atopic Dermatitis or eczema:
Atopic eczema (or atopic dermatitis) may have a genetic component and tends to be found in families with a history of hay fever and asthma. It usually appears on the face, scalp, neck and on the side of the limbs in infants, as well as inside the elbows and behind the knees in older children and adults.
Contact dermatitis occurs in two forms: allergic and irritant. Allergic contact dermatitis is usually a delayed reaction to an allergen, such as poison ivy. Irritant contact dermatitis is more common and is the result of a reaction to an irritant. For example, sodium lauryl sulfate (found in some personal care products such as shampoo, soaps and toothpastes) is one of many solvents that can cause skin irritation.
Xerotic eczema, also known as winter itch, begins as dry skin, usually on the limbs and trunk, and becomes so severe it turns into eczema. This condition occurs most commonly in the elderly, but young people can also develop it.
Seborrhoeic dermatitis is often referred to as dandruff, or cradle cap in infants, and affects the scalp and eyebrows and at times along the sides of the nose.
There are other, less common, forms of Atopic Dermatitis as well:
- Dyshidrosis is typically seen on the palms, soles of feet and sides of fingers and toes. It is characterized by tiny fluid-filed blisters (vesicles), thickening and cracks that itch, especially at night. Warm weather and stress make the condition worse.
- Discoid eczema most frequently appears on the lower legs as round patches of dry, cracked skin that sometimes oozes fluid. The cause is unknown.
- Venous eczema, or stasis dermatitis, is most commonly seen in people over 50 with poor circulation, varicose veins and edema (swelling). It is characterized by redness, itching, and darkening of the skin.
- Autoeczematization, or “ids,” usually occurs as a result of an infection by parasites, fungi, bacteria or viruses and always develops some distance from the initial infection. The type of infection that causes this condition determines how it looks, so the appearance of autoeczematization varies. The only way to cure it is by eradicating the initial infection.
- Neurodermatitis develops when persistent scratching irritates the skin. It is thought to have emotional or “nervous” causes. This condition is controlled with antihistamines and corticosteroids as well as behaviour modification (e.g., learning to stop habitual scratching).
Fast Facts
- Atopic Dermatitis is one of the world’s most frequently diagnosed skin conditions.
- It is particularly common in young children and infants: 10 to 15 per cent of Canadian children under 5 are affected.
- Though some infants outgrow the condition by their second birthday, 40 per cent live with it throughout adulthood.
- About 10 to 20 per cent of the population lives with Atopic Dermatitis in one form or another.
- The number of people with Atopic Dermatitis in Canada is higher than the worldwide average.
Looking Deeper
There are two theories about the causes of Atopic Dermatitis. The first is that a person with atopic dermatitis is predisposed to excess inflammation. This is caused by the type of inflammatory cells present in the skin, the types of chemicals these cells make, and the way they communicate with other cells. The excess inflammation caused by these cells and their chemicals leads to itchy, red, swollen skin, which sets the stage for irritation and infection. The second theory is that a person with atopic dermatitis has skin that does not provide the same protection as a healthy person’s skin. This allows foreign molecules to gain entry to the skin’s deeper layers, provoking inflammation, which causes skin itching and redness. Both theories are most likely interlinked. The causes of atopic dermatitis are still not fully understood; fortunately, international and Canadian dermatology researchers continue to work on this puzzle.
 atopic dermatitis-1
atopic dermatitis-1  atopic dermatitis -2
atopic dermatitis -2  atopic dermatitis-3
atopic dermatitis-3  atopic dermatits-4
atopic dermatits-4
Symptoms
Slightly different symptoms and clinical signs exist for each type of atopic dermatitis, and they can range in terms of severity and location on the body. However, the first symptom of atopic dermatitis is usually intense itching, followed by a patchy, flaky, scaly, dry, hot, inflamed skin rash. Other atopic dermatitis symptoms and clinical signs include:
- Repeated rashes
- Redness
- Swelling
- Crusting
- Scabbing
- Blistering
- Cracking
- Oozing
- Bleeding
As there are different types of atopic dermatitis, so too are there different triggers, which can range from chemicals, bacteria, allergens, side effects of medications and psychological factors. Some triggers include:
- Soaps and detergents
- Cosmetics
- Weather conditions (heat, cold, humidity, dryness)
- Environmental allergens (such as poison ivy, ragweed, and primrose)
- Jewellery
- Creams
- Food handling
- Clothing (due to the chemicals used in manufacturing)
- Sweating
- Gloves
- Rubbing
- Emotional or mental stress
Flare-ups can be caused by:
- Illness
- Unusual physical or mental stress
- Exposure to skin irritants
- Skin infections
Treatment
Learning the cause of atopic dermatitis isn’t always easy due to the number of possible triggers and the many types of the condition. However, in all cases, a doctor will use the location of the initial rash as a first clue.
For contact dermatitis, a doctor may perform patch testing, which consists of placing small patches on the skin. These patches contain substances typically known to cause the condition. This type of testing can be difficult to interpret as doctors need to select which substances to test, and the results may not always be accurate.
With atopic dermatitis, a physician will explore your medical history and often whether your family members have allergies. This will help identify possible triggers.
For neurodermatitis, your doctor will look to discover any underlying psychological stressors, allergies, or, depending on the rash location, other underlying medical conditions, such as fungal infections, warts or psoriasis.
Although no cure exists for atopic dermatitis, a number of treatment options are available for relieving the inflammation and itching that it causes. The treatments range from lifestyle changes and skin-care strategies to medication.
Lifestyle changes and skin-care strategies
Keeping your skin hydrated is one way to control atopic dermatitis. It is best to hydrate when you wash because bathing allows rough skin to soften, take in water, and better absorb the topical treatments you apply. When bathing or showering, use lukewarm water (not hot). After bathing or showering, lightly pat your skin with a towel. Then apply your prescription ointments or creams and, once they’ve been absorbed, a good moisturizer.
There are many classes of moisturizers. The least effective are lotions or creams; the most effective moisturizers are ointments. It’s usually best to use ointment-type moisturizers during a flare-up and only after you've applied your prescription ointment. When the skin is clear, you can move back to a fragrance-free lotion.
Short, frequent, gentle bathing or showering also washes away Staphylococcus aureus, a bacterium that is found on everyone’s skin and seems to be attracted to atopic dermatitis. Some people with atopic dermatitis can also develop an allergic reaction to this bacterium, which can worsen their condition.
Preventing flare-ups is another effective way to control the condition. Here are some tips to help you to avoid triggering symptoms:
|
AVOID |
INSTEAD |
|
|
Medical Treatments
Treatments for atopic dermatitis generally fall into two categories: those that control symptoms such as itching or dryness, and those that modify the immune system or decrease inflammation. Proper skin care and over-the-counter treatments, as described above, may be enough to control mild cases of atopic dermatitis. If these fail, your doctor may prescribe a topical treatment, such as a medicated cream or ointment, for moderate atopic dermatitis, or a systemic treatment (in pill form) for severe or widespread cases.
Topical treatments (creams, lotions, ointments)
Calcineurin inhibitors are found in creams or ointments containing tacrolimus or pimecrolimus, both of which are immune-modifying drugs. These drugs work by reducing inflammation in the skin. A thin layer of the cream is applied to the affected area twice daily. To avoid rare side effects, these products should not be used continuously over a long period of time, or in children under age 2. You should also minimize exposure to natural (e.g., sunshine) and artificial (e.g., tanning beds) ultraviolet light. Common side effects include a burning feeling or warmth at the application site, which is of short duration and usually disappears after the first week of use.
Corticosteroids are synthetic versions of hormones made in the body. When applied to the skin, they reduce inflammation in the area, making them useful treatments for some forms of atopic dermatitis. Apply the cream sparingly to the affected skin with a gentle massage, 3-4 times each day. Decrease or discontinue the use once the condition is under control. Side effects include dryness, itching, burning and local irritation. Excessive use of corticosteroids (i.e., for an extended period of time over a large area of skin) may cause hormonal problems in rare cases. It is important to follow any instructions your doctor gives you.
Emollient creams/ointments are over-the-counter topical products used to soften and moisturize the skin and help preserve its function as a barrier to water loss. These products may be soothing and help remove dry, scaling skin, as well as increase the effectiveness of other topical treatments. These can be applied generously to affected and unaffected areas.
PDE4 inhibitors are enzymes that help to regulate inflammation in your body. When you have atopic dermatitis, PDE4 enzymes may be overactive in your skin cells. This can lead to inflammation of the skin. The only approved drug of this type is Eucrisa (crisaborole), the first topically applied PDE4 inhibitor to be approved by Health Canada for use for adults and kids as young as 2 years old living with atopic dermatitis. It was developed as a small-molecule, boron-based, selective PDE4 inhibitor that can be used topically. Unlike PDE4 inhibitors that act systemically, this treatment does not cause significant gastrointestinal adverse effects. The most common side effect is stinging and burning when the product is applied to the skin.
Systemic treatments (for very severe atopic dermatitis)
Corticosteroids can also be injected. When taken in this manner, they alter the body’s immune response, reducing inflammation in the skin and elsewhere. As with the topical creams, corticosteroids can cause changes in the body’s hormone production if used excessively. Your doctor will carefully plan the dosing and duration of treatment to avoid this. Less severe side effects include weight gain, nausea or vomiting.
Cyclosporin, a drug used to treat people who have had transplants, has been shown to be effective in people with severe atopic eczema, especially where their lives are significantly disrupted by their condition. The drug is believed to work by suppressing severe allergic and immune reactions. Since it is very powerful, it tends only to be prescribed for a small percentage of patients.
In addition to the medications described above, new treatments not yet on the market are being tested regularly.
Biologics
Biologics (or biosimilars) are medications that are produced from living cells, such as animal cells, bacteria, or yeast. They target specific parts of a person’s immune system to treat diseases such as psoriasis, psoriatic arthritis, rheumatoid arthritis, and some cancers. People can receive biologics through an injection or an intravenous (IV) infusion. The only approved drug of this type is Dupixent (dupilumab) for adult patients living with moderate to severe atopic dermatitis. Common side effects include cold sores, dry eyes and redness at the injection site.
Other Treatments
Medications officially approved for treating other conditions/diseases have been tried in eczema with variable success. They are included here for information only.
Phototherapy is a treatment in which the skin is exposed to ultraviolet light, slowing the growth of affected skin cells. There are two forms commonly used to treat severe atopic dermatitis :
- PUVA (psoralen/ultraviolet A): a drug called psoralen is given (either as pills or applied to the skin) that sensitizes the skin cells to ultraviolet A light. Psoralen pills can cause nausea, vomiting, headaches and sensitivity to UV light (including sunlight)
- UVB (ultraviolet B): uses ultraviolet light (B form) only
Both types of phototherapy are performed at your doctor’s office. As with repeated exposure to natural UV light from the sun, repeated use of phototherapy over a long period of time can lead to drying and ageing of the skin and may increase the risk of skin cancer.
Wet wraps
Wet wraps are a treatment that uses a low-potency topical steroid and an emollient (moisturizer) to calm flares and improve the effectiveness of the medication. It is often used for those with moderate-to-severe atopic dermatitis, especially children, where topical applications have not helped. Wet wraps involve double layers of tubular bandages forming a body suit. They work in two ways:
- Evaporation cools the skin, reducing itching and discomfort. If the bandages become dry, you can remoisten them (this is usually only needed for an overnight treatment).
- Rehydration puts moisture back into the skin as the skin absorbs large amounts of the product. It also improves the penetration of the medication into the skin.
How to perform a wet wrap:
- Cover your chair or sofa with plastic or a garbage bag. Make sure to have a TV or good book within reach!
- Moisten a cloth with room temperature water, wring it out, and set aside. For small treatment areas you can use a washcloth; an old t-shirt or an old pair of long-sleeved and long-legged pyjamas work well for larger areas. Tubular sleeves work as well if you have them.
- Generously apply the prescribed medicated ointment or cream to the affected areas.
- Wrap the areas with the damp clothing/towel, make yourself comfortable with a large blanket, and leave the wrappings for at least 1 hour – it can even be done overnight.
- Remove the coverings and immediately apply a generous amount of an unscented moisturizer all over the body.
- Ideally, continue the procedure twice a day to get flare-ups under control.
Coal tar applied to affected areas has been shown to help reduce the itchiness of atopic dermatitis. But its strong smell and tendency to stain any fabric it touches make it a less appealing remedy. Coal tar can also irritate the skin in some people. It should only be used under the guidance of a doctor with experience in managing atopic dermatitis.
*All information on medical treatments on this site is provided as an overview only. For a complete and up-to-date list of side effects, warnings and precautions, read the product’s package insert and consult your doctor or a pharmacist.
**If you are considering an alternative or complementary therapy, discuss it with your doctor first, and always be sure to keep your doctor up to date about any vitamins, supplements, or other forms of alternative treatment you are taking. Like any medication, alternative therapies can interact with other medications/treatments and, in some cases, have side effects of their own. Remember that “natural” does not necessarily mean “safe.”
Coping and Support
Atopic dermatitis has been called the condition you “wear” as it affects your appearance. And while the clinical aspects of atopic dermatitis are obvious, the psychological effects may not be. Symptoms such as redness and flaking can be severe and, when visible to others, can cause some people to be self-consciousness. As well, friends, family and colleagues may not understand this condition, and their lack of sensitivity may upset those with atopic dermatitis.
In addition, the pain and itching associated with atopic dermatitis can be a particular problem at night when it disrupts sleep. Lack of sleep can have repercussions for daily life and interfere with the ability to function well mentally at work or school.
School children particularly may feel embarrassed if they are teased by their classmates because of their condition. As a result, they can experience isolation, low self-esteem, and poor school performance. Parents must be aware of these risks and encourage their children to understand their eczema, be comfortable with it, and talk to their peers about it.
Acknowledging that you have eczema and that it will likely be part of your life for a long time is an important step to managing your well-being. In addition, learning how to control symptoms and keep flare-ups in check through a simple daily skin-care routine can help ease your stress.
Here is a link to a recent report (The Skin I'm in: A NATIONAL REPORT OF THE PATIENT AND CAREGIVER EXPERIENCE WITH ATOPIC DERMATITIS) that we completed in 2017 on the patient and caregiver experience with atopic dermatitis.
Other associations can also help. Visit theEczema Society of Canada or the National Eczema Association (NEA) websites for news, information and advice.
Resources
If you are living with Atopic Dermatitis or know someone who is, you may want to stay up-to-date on the condition as well as current treatments and news.
Our Affiliate Members

Resources:
Eczema Resources for Kids

Atopic Dermatitis Brochure Atopic Dermatitis Infographic


The Skin I'm In Infographic My Life with Atopic Dermatitis My Child Has Atopic Dermatitis
Canadian Skin Articles on AD:
Websites:
Reports:
Videos:
Birthmarks
Overview: What are birthmarks?
The information in this section has been gathered from existing peer-reviewed and other literature and has been reviewed by expert dermatologists on the CSPA Medical Advisory Board.
Birthmarks are patches of discoloration or abnormal texture on or under a person’s skin. Sometimes these marks appear soon after a baby is born, but most are obvious at birth. In some cases, the birthmarks fade or disappear altogether as the child gets older, but others stay the same or actually get bigger, darker, or thicker. In many cases, birthmarks are both harmless and painless, but facial birthmarks can be a source of stress for people who have them. Some birthmarks, especially those that are larger, may be associated with internal medical conditions that may require evaluation and treatment.
Birthmarks come in a variety of sizes, shapes, and colours. The colour, for example, can range from blue or blue-grey, to brown, tan, black, pink, white, red, or purple. Many birthmarks are soft, raised swellings on the skin; others are smooth. Birthmarks can occur anywhere on the body. The two most common classes of birthmarks are:
- Red birthmarks, which are usually caused by extra blood vessels clustered together close to the skin surface and are called vascular birthmarks.
- Pigmented birthmarks, which are due to abnormally increased amounts of melanin in the skin. Melanin is the main pigment that gives skin its colour.
It is not known exactly why some children develop birthmarks and others do not.
 Cafe au lait macule
Cafe au lait macule  Congenital mole
Congenital mole  Hemangioma
Hemangioma  Port wine stain
Port wine stain
Symptoms
Stork Bite or Angel’s Kisses: These tend to be pink, irregularly shaped, and flat, less than a few inches inches tall and wide, and usually found on the neck, head, or upper lip. Almost half of all newborns have one of these birthmarks. There are no known health problems associated with them, and they usually fade by the end of the first year.
Infantile Hemangioma: These are usually red, raised, and lumpy, and may be several centimetres across. They can appear anywhere on the body and occur in one in 20 births. These marks commonly appear between one and four weeks after birth; they can then grow quite rapidly before stopping and slowly fading. Fifty per cent of these marks vanish by the age of five, and 90 per cent have gone by the age of nine. Where the hemangioma is blocking vision or breathing (rare), oral medications (known as beta-blockers), surgery, or laser treatment may be recommended.
Port-wine stains (nevi flammeus): These are usually pale pink at birth but become darker red with time, sometimes appearing like the colour of red wine. They typically occur in three in 1000 births. The shape is irregular, and these stains can sometimes be very large. When they occur on the face, they can make people feel self-conscious. Port wine stains are usually considered permanent and will not generally fade, and those around the eye and forehead can be associated with glaucoma. Port wine stains can also occasionally appear with Sturge-Weber syndrome, a rare disorder where abnormalities may also appear in the brain and eyes.
Congenital Dermal Melanocytosis: A bluish, bruise-like, irregular, flat birthmark, Mongolian Spots are typically about 10 cm across and found on the lower back and buttocks. They are most frequently seen among darker-skinned people, particularly among those from East Asia. Mongolian Spots may not appear until sometime after birth, but gradually fade over several years. They have been mistaken for abuse bruises by social workers and health care professionals.
Café au Lait Spots: Most commonly a light brown, milk-coffee colour, and oval to round, these can appear anywhere on the body and usually include only one or two spots. There are no health problems associated with one or two spots, but if there are many of these spots there is a possibility of neurofibromatosis. Café au Lait spots do not fade with age.
Congenital melanocytic nevus: These usually appear as brown to dark-brown marks that may only be slightly raised, although larger ones can be raised and lumpy. They range from less than 1 cm to more than 30 cm and can appear anywhere on the body. Sometimes congenital melanocytic nevi can be hairy. The marks occur in about one in 100 births. It has been suggested by some studies that there is a cancer risk associated with the larger marks. These large visible marks can have a psychological impact. Surgical removal is an option, but will usually lead to scarring. The marks should be watched for any changes that could indicate cancer.
Treatment
Birthmarks are easily identified by parents and doctors. In some cases, they can indicate an underlying, more serious condition. For this reason, it is a good idea to have your doctor check your child’s birthmarks.
A few birthmarks may resolve on their own by simply fading away. Most, however, will generally be permanent. Surgery or laser treatment may be treatment options, but these should be approached cautiously since scarring may occur. There is a growing body of experience among dermatologists in treating birthmarks, and sophisticated new treatments combining laser therapy with other forms of light seem effective.
Some types of birthmarks may respond to medication. For example, oral beta-blockers or steroids can be taken to reduce the size of infantile hemangiomas. However, as with any medication, the side effects must be weighed against its benefits.
Some smaller or lighter birthmarks may be effectively covered with cosmetic camouflage cream.
Coping and Support
Society emphasizes physical appearance, so having a visible birthmark can really make a person stand out. Children may be particularly sensitive to such treatment. Your and your child’s reactions to how others act when they see the birthmark is important. Here are some ideas for helping you or your child:
- Be positive about people’s reactions. People are often curious and do not know how to react to a visible birthmark. Accept that they are not being rude and try to be polite, friendly or even humorous. It may help to explain the type of birthmark you have. Also, it is okay to be assertive. If other people’s questions seem intrusive, it is all right to let them know.
- Talk to your child about his or her birthmark. Be open, honest, and calm. Use simple terms they can understand. Explain any treatments that they might be getting in the future.
- Show your child how to cope. Children learn by watching other people, especially their parents. Your child will learn how to handle things like hospital visits, making friends, and coping with other people’s reactions by watching you. Therefore, the best way to teach your child is to learn how to respond well to people yourself.
Most birthmarks pose few or no problems, but a person who has a large, obtrusive birthmark on the face may feel very self-conscious. If it’s a child who has the birthmark, parental encouragement and support may be all that’s needed. However, during puberty, the power of parents’ help begins to wane, and the perceptions of others becomes more significant. (For example, unafflicted girls may reject or isolate a peer with a birthmark because they may not want their “blemished” friend to “scare away” boys.) The emotional scars developed during this time may remain with the person for life. As a parent, the best thing to do is to maintain an open dialogue with your child, be as supportive as you can, and consult dermatologists about available treatment options.
For those people with birthmarks who may be limiting their social interactions with others, the support of a psychologist or counsellor may help.
Resources
If you are living with birth marks or know someone who is, you may want to stay up-to-date on the condition as well as current treatments and news.
Our Affiliate Member
.  AboutFace, at http://aboutface.ca/, provides support for people with facial differences.
AboutFace, at http://aboutface.ca/, provides support for people with facial differences.
Other Resources
To learn more about birthmarks, the National Organization of Vascular Anomalies (NOVA) or the Vascular Birthmarks Foundation can be a source of information
Burns
Overview: What is a burn?
The information in this section has been gathered from existing peer-reviewed and other literature and has been reviewed by expert dermatologists on the CSPA Medical Advisory Board.
A burn is a type of skin injury that occurs when the skin or other tissue is damaged by coming in contact with:
- Chemicals, such as acids or alkalis (pronounced al-ka-lies)
- Very hot surfaces, liquids, foods, air or steam
- Fire
- Radiation, such as overexposure to x-rays and sunlight
- Electricity
- Hard surfaces, causing a friction burn
Although the skin is usually the area that is burned, the tissues underneath and internal organs can also be affected. Health-care professionals determine the severity of a burn based on how deep it goes and how much of the body it covers: the deeper and more widespread a burn is, the more serious it is. Burns are generally categorized as first, second, third or fourth degree. Many burns are superficial and, although painful, heal quickly and easily. However, very severe burns can be life-threatening and cause significant scarring.
Symptoms
The one symptom that all burns share is swelling, which usually begins to subside in about 48 hours. However, other symptoms can persist longer than two days and vary according to how serious the burn is.
First-degree burns are superficial, considered mild, and have similar characteristics to a sun burn, affecting only the first layer of skin (the epidermis). These burns cause skin redness and pain. They generally heal in 3 to 5 days, although in some cases the redness may last longer.
Second-degree burns fall into two types:
- Superficial partial-thickness burns, which injure the first and second layers of the skin (epidermis and superficial dermis)
- Partial-thickness burns, which injure deeper skin layers (epidermis and most of dermis, including deep follicular structures).
Unlike first-degree burns, second-degree burns cause blistering or open sores on the skin, are more painful than first-degree burns, and take 10 to 15 days to heal. If you have a second-degree burn, you should see your doctor. Seek immediate medical help if the burn is larger than 2 or 3 cm in diameter or is on the face, hands, feet, genitals, buttocks, or a major joint.
Third-degree burns (full-thickness epidermal and dermal destruction) are more serious than first- and second-degree burns because they extend through all of the skin’s layers. The skin dies, turns white and has no sensation because of damaged nerve endings. A skin graft is necessary to heal the area. People with third-degree burns that cover a large part of the body can go into shock, stop breathing and die. Anyone with suspected third-degree burns needs to be immediately taken to hospital.
Fourth-degree burns (extends through skin, subcutaneous tissue and into underlying muscle and bone). People with widespread fourth-degree burns can die from their injuries. This type of wound leaves the body vulnerable to infections. Reconstructive surgery is needed to repair the burned area.
Important note: Third- and fourth-degree burns, or burns that cover more than 10% of the body, must always be treated at a hospital.
Treatment
Treatment for burns depends on the severity of the injury and ranges from immediate attention (first aid) and over-the-counter creams to prescriptions, emergency medical care and ongoing management.
First Aid
First- and Second-degree Burns
Applying first aid to first- and second-degree burns is an important step to healing properly:
- Act quickly!
- If the victim is a child or an adult over 70, seek immediate medical assistance.
- First- and second-degree burns should be run under cool water for at least 15 minutes.
- NEVER apply ice or butter to burns or break any blisters because you risk further damaging the skin.
- Cover the affected area with a sterile bandage.
After applying first aid, less severe burns can usually be treated at home:
- For adults, use pain medication as needed. For children, use the pain medication recommended by hospital medical staff.
- Second-degree burns can be treated with prescription antibiotic creams or pills, as well as painkillers.
Third- and Fourth-degree Burns
Knowing what to do when someone suffers a serious burn can save his or her life. Below are the first-aid procedures for third- and fourth-degree burns:
- Call 911 and perform CPR if there are no signs of breathing and a pulse.
- Elevate the burns above the heart, if possible, and cover them with a cool, moist, sterile bandage or a clean, moist cloth or towel.
- NEVER remove burned clothing or immerse severe burns in cold water.
Once first-aid treatment has been applied and the person with the burn has been assessed by a physician, longer-term burn treatment can begin. Specialized treatment for severe burn cases may include:
- Placement of a breathing tube if the person’s airways or lungs have been damaged by hot air or flames
- Administration of fluids through an intravenous tube
- Immunization with tetanus vaccine and use of antibiotics to prevent infection
- Covering the burned area with antibiotic ointments and bandages
- Debridement, or removal of dead tissue
- Skin grafting, a procedure done in an operating room that involves transferring a patch of non-burned skin to the burned area
- Physical and occupational therapy to keep burn areas flexible and to manage scarring
- Made-to-fit elasticized pressure garments to minimize the amount of scarring following a burn injury by decreasing hypertrophic (excessive) scar growth; they generally need to be worn for one to two years following the injury.
The goals of burn treatments include relieving pain or itching, preventing infection and minimizing permanent scarring. Many burn treatments are available without a prescription.
Topical Treatments (Creams, Gels, Ointments)
 Bacitracin is an antibiotic cream or ointment applied to the skin to help treat and prevent infection and aid in the healing of burns. A small amount is applied to the (clean) affected area, 1-3 times daily, for up to a week. Do not use bacitracin if you are sensitive or allergic to this type of antibiotic.
Bacitracin is an antibiotic cream or ointment applied to the skin to help treat and prevent infection and aid in the healing of burns. A small amount is applied to the (clean) affected area, 1-3 times daily, for up to a week. Do not use bacitracin if you are sensitive or allergic to this type of antibiotic.
Silver sulfadiazine is a prescription antibacterial cream used for treating burns, especially for treating and preventing infection of serious burns. Each day, after cleaning the wound, apply a 3-5 mm-thick layer of cream. The cream should not be used during the late stages of pregnancy or in premature or newborn infants. The cream may affect scabbing and/or the appearance of the burn wounds. Common side effects include burning, rash or itching where the cream is applied. Leukopenia (low white blood cell count) is also common; careful monitoring of the blood is required.
Systemic Treatments
Analgesics (e.g., acetaminophen/paracetamol) offer temporary relief of mild to moderate pain. Acetaminophen  and ibuprofen are available without a prescription. The pills or capsules are taken orally as needed, with doses separated by 4-6 hours. Some people may experience nausea, heartburn, dizziness and rash as side effects. An overdose of acetaminophen can cause serious liver damage.
and ibuprofen are available without a prescription. The pills or capsules are taken orally as needed, with doses separated by 4-6 hours. Some people may experience nausea, heartburn, dizziness and rash as side effects. An overdose of acetaminophen can cause serious liver damage.
Diphenhydramine is an antihistamine available in pill form without a prescription that can be used to treat severe itching. This medication should be taken orally, as directed (usually every 4-6 hours). A side effect is drowsiness.
New medications and treatments are regularly being tested for burns. To learn about the latest in burn care, visit our clinical trials page [link to CSPA clinical trials page].
Ongoing Management
If you are recovering from a burn, see a doctor when you need help controlling the pain or are unsure of how to care for your burn.
A person who is burned is often left with a scar after the skin is done healing. If a person has had a skin graft to heal the burn, that site may also scar. Depending on how bad the burn was, the scar may be hardly noticeable or very noticeable.
{jkefel title=[Looking Deeper]}
Scar tissue is made of collagen, the tough material manufactured by fibroblasts (the fibre-making cells that rebuild all injuries). In smaller cuts, we cannot see the small amount of collagen fibre that forms beneath the surface of skin. However, the large amount of fibre that is needed to close a large wound creates a visible scar. Because scar tissue is made of fibres, not regular skin cells, it is stronger than ordinary skin and may look shiny, with a colour different from the non-injured skin (usually pink or red). As well as being a different colour, some burn scars are itchy and may appear lumpy or raised.
Burn scars can take from up to two years to “mature” or finish changing. The colour of a mature scar is usually close to the skin’s original colour; the scar does not itch and is no longer painful. Skin that is mature is softer and moves more easily than before. With the proper therapy, the burned skin can heal with the least amount of scarring possible.
During healing and in cases where the burn area crosses a joint, physical therapy is necessary to keep or regain movement that may have been lost due to the tightening of the healing skin. Burn patients may need to wear splints to keep their joints in a stretched position to prevent them from tightening.
{/jkefelend}
Footnote:
*All information on medical treatments on this site is provided as an overview only. For a complete and up-to-date list of side effects, warnings and precautions, read the product’s package insert and consult your doctor or a pharmacist.
**If you are considering an alternative or complementary therapy, discuss it with your doctor first, and always be sure to keep your doctor up to date about any vitamins, supplements, or other forms of alternative treatment you are taking. Like any medication, alternative therapies can interact with other medications/treatments and, in some cases, have side effects of their own. Remember that “natural” does not mean “safe.”
Coping and Support

People who suffer severe burns may take years to recover physically and emotionally. Each burn survivor copes with his or her injury differently, depending on how serious the
burn is and the person’s personality. Along with the physical pain and change in appearance, a burn survivor may experience loss (e.g., temporary or permanent leave from work, inability to care for family, being unable to engage in leisure activities), fear about the future, anxiety about recovery and concern about returning to a normal life.
There are two important factors that have consistently been found to influence psychological and social adjustment following burn injuries: the enduring quality of family and social support received by the burn survivor and the willingness on the part of the survivor to take social risks.
Conversely, factors associated with poor psychosocial adjustment by a burn survivor include:
- Social shyness
- An acceptance within the family of the survivor’s dependence (learned helplessness)
- Lack of family cohesion and high conflict within the survivor’s family
A full physical and psychological recovery from a serious burn can be a difficult process and involves major adjustments as a survivor works to develop a new life, a new body image, and new ways to feel confident. Some strategies for recovering emotionally from a severe burn include the following:
- Include all members of the family in all aspects of treatment.
- Practise autonomy: doing things for yourself in a new way.
- Learn to manage predictable reactions from naïve observers (e.g., staring, questions about what caused the burn).
- Practise social skills and social risk-taking. James Partridge, director of Changing Faces, an organization that assists people with facial disfigurement, recommends adopting a social skills technique called “3-2-1-GO!” in which the survivor plans for uncomfortable social situations by thinking of 3 things to do when someone stares at them, 2 things to say when someone asks them what happened (to cause their scars), and 1 thing to think if someone turns away from them. Other coping techniques include going out with family members or friends to feel less conspicuous and reminding yourself that who you are on the inside has not changed, your skin will continue to heal up to two years after the burn and the scars will become less obvious over time.
- Identify positively as a burn survivor, rather than as a burn patient or victim.
- Celebrate rehabilitation gains and social accomplishments.
- Understand that each burn survivor is a human being who can be strong and competent, optimistic and autonomous, but also experience moments of sadness, despair or rage.
- Remind yourself that soon you will be comfortable in a new routine, or a “new normal” life. There will be life after the hospital, after the end of rehabilitation and after the pressure garments come off! This new life can be just as good or even better than the one that existed before the burn.
- Be prepared for the emotions at various phases of recovery.
- Connect with others who have had similar experiences. Some hospitals and associations run support groups.
Resources
If you are a burn survivor or know someone who is, you may want to stay up-to-date on the condition as well as current treatments and news.
Our Affiliates


Other Resources
- Columbia Professional Fire Fighters’ Burn Fund
- Calgary Firefighters Burn Treatment Society
- Calgary Burn Survivor Group, This email address is being protected from spambots. You need JavaScript enabled to view it., Burn Survivor
- Camp Mamawi, Burn Camp for Children, This email address is being protected from spambots. You need JavaScript enabled to view it., Director
- Camp Bucko, Burn Camp for Kids in Ontario
- Cape Breton Firefighters Burn Care Society
- Firefighters Burn Treatment Society, Edmonton Chapter
- Nova Scotia Fire Fighters Burn Treatment Society
- Saskatchewan Professional Fire Fighters Association Burn Fund
- This email address is being protected from spambots. You need JavaScript enabled to view it.
Cancer: Melanoma
Overview: What is skin cancer: melanoma?
The information in this section has been gathered from existing peer-reviewed and other literature and has been reviewed by expert dermatologists on the CSPA Medical Advisory Board.
Melanoma is a cancer that begins in the pigment-producing cells (melanocytes) of the skin. It is considered the least common yet the most serious of the three main types of skin cancer, which also include basal cell and squamous cell cancers [link to skin-cancer: non-melanoma section].
Skin cancer results from cells that multiply out of control. As a result, tumours, lumps, or masses can sometimes form on normal skin, and can be either benign (non-cancerous) or malignant (cancerous). Some types of cancer are more likely than others to spread to other parts of the body and cause damage. This process is called metastasis. Melanoma is considered the most serious type of skin cancer as it may spread where it continues to grow and destroy tissue. If it is detected early, most melanomas are curable.
In its earliest stage, melanoma is confined to the outer layer of skin (the epidermis) and is known as in situ melanoma. If the melanoma goes undetected, it can grow deeper, penetrating the middle layer of skin (the dermis). At this stage, it is known as invasive melanoma.
There are four types of melanoma:
Superficial spreading melanoma (SSM) is usually diagnosed when people are in their 40s or 50s. It represents approximately 70 per cent of all melanomas. SSM can arise from a mole or on otherwise normal skin and most commonly occurs on the upper back in men and the upper back or legs in women. SSM usually looks like a deeply pigmented flat or slightly raised area.
Nodular melanoma (NM) accounts for 15 to 30 per cent of all cases. It most often appears in midlife, usually on the person’s trunk, head, or neck. The onset can be rapid, with NM often developing within several months. Unlike other types of melanoma, it is invasive from the onset and typically appears either as a uniform dark blue-black or bluish-red area, or as an area without any pigment.
Acral lentiginous melanoma (ALM) represents the most common form of melanoma in darker-complexioned people and Asians but occurs less frequently in people with light complexions (only 2 to 8 per cent). ALM occurs on the palms of the hands, soles of the feet, or beneath the nails. It can appear as a tan, brown or black flat lesion with changes in colour and irregular borders. It may often be under the nail as a brown to black discolouration. Most cases involve the big toe or thumb.
Lentigo maligna melanoma (LMM) has been likened to a stain on the skin. At the beginning, lentigo maligna (LM) is confined to the epidermis. If it extends into the dermis, it is termed LMM and is the least common type of melanoma. LM and LMM are almost always found on areas of the skin that have had long-term sun exposure, such as the nose, cheeks, head and neck. LMM most often occurs in older patients, beginning in the 60s. Frequently, the lesion is quite large (3–6 cm or larger). The colours in flat areas include tan, brown, black, blue-grey and white.
The risk of developing a melanoma is greater if a person has a family history of skin cancer, has a lot of moles, or has fair or freckled skin, blue eyes and light-coloured or reddish hair. However, anyone who has had excessive sun exposure, severe and frequent sunburns during childhood, or has lived in a sunny or high-altitude climate is at increased risk of developing skin cancer.
As with many other skin conditions, preventing melanoma is better than a cure. To reduce your risk, you should:
- Avoid prolonged sun exposure, especially between 11 a.m. and 4 p.m.
- Don’t use tanning beds or sun lamps.
- Apply sunscreen that has an SPF of 30 or higher and that protects against UVA and UVB rays, even in the winter. Reapply after swimming or sweating.
- Wear protective clothing, such as closed-toed shoes, hats that shade your face, long pants and long sleeves.
- Seek shade when you’re outside.
Symptoms
Melanoma can begin as a small, pigmented growth on normal skin, most often on sun-exposed areas, yet nearly half of the cases develop from existing moles. It commonly occurs on the backs of men and legs of women, but it can occur anywhere on the body where melanocytes (pigment-producing cells) are found, including the eyes, mucous membranes (mouth and genitals), and internal organs.
This type of cancer is generally treatable if caught early, so check your body monthly for new pigmented spots or changes in existing spots that exhibit the A-B-C-D-Es of melanoma:
- Asymmetry (the shape is not symmetrical)
- Border (the border is irregular)
- Colour (the colour has uneven, irregular brown or black pigment. There may be blue-black, red, blue or white areas)
- Diameter (the diameter is larger than 6 mm; however, many melanomas are smaller than 6 mm in diameter, and it is best to find them before they reach this size)
- Evolving: the pigmented lesion is changing in size, colour, or shape
Melanomas generally cause no symptoms. If melanoma has metastasized (i.e., spread to other parts of the body), you can develop swollen lymph nodes, a colourless lump or thickening under the skin, unexplained weight loss, grey skin, an ongoing cough, headaches or seizures.
Treatment
To diagnose melanoma, a doctor will take your medical history and perform a physical exam. If melanoma is suspected, your doctor will take a biopsy—usually right in the office—(either of the entire mole or a small sample of it) to confirm the cancer. If it is melanoma, the skin sample may be studied further to look for specific features that may provide information about prognosis.
If your doctor suspects that the melanoma has spread deeper into the skin, she or he may order other tests such as a biopsy of nearby lymph nodes, x-rays, scans, or blood tests.
Following a confirmation of melanoma, your doctor may consult with or refer you to other professionals for treatment, including a dermatologist, plastic surgeon or oncologist.
Generally, the earlier that melanoma is caught, the more successful the treatment will be. However, the outcome will depend on tumour thickness, ulceration and depth, the location of the cancer, the severity (or stage) of cancer, and a person’s age. The less melanoma has grown into the skin, the better the chance of curing it.
There are five common treatments for melanoma:
Surgery to remove the tumour is the main treatment for melanoma at all stages and there are several different types:
- Excision to remove the tumour and surrounding skin
- Sentinel lymph node biopsy to remove the first lymph node likely to be invaded if the melanoma metastasizes
- Lymph node dissection, which removes all lymph nodes close to the tumour, particularly those that can be felt by physical examination; this surgery causes long-lasting, uncomfortable fluid build-up and is done only if necessary
Radiation therapy uses high-energy rays or particles to kill cancer cells. It is most often used in advanced cases of melanoma that have spread to the brain or bones. In external beam radiation therapy, a machine directs radiation to the tumour and surrounding area. Radiation therapy may be used as the therapy of choice if a person’s health will not tolerate surgery, if a recurring tumour’s location or size makes surgical removal cosmetically unacceptable, or if there is a high risk of recurrence. Radiation therapy to lymph nodes can scar lymph nodes and block fluids, leading to fluid build-up.
Chemotherapy uses cytotoxic (cell-killing) drugs to remove cancer cells. Limb perfusion, or isolated limb perfusion, is used to deliver medication directly to the affected limb. With this technique, blood flow to the limb is stopped using a tourniquet and the medication is injected directly into the limb. This may be used to treat melanoma believed to have spread to the arm or leg.
Systemic drug treatments are also used for this type of cancer. Common systemic agents are dacarbazine, given singly by intravenous infusion, and temozolomide, given singly by oral dose, or a combination of vinblastine, cisplatin and dacarbazine (a combination known as CVD) by intravenous infusion.
Biological therapy (immunotherapy) uses natural or manufactured agents to strengthen the immune system. Biological therapy may be used after surgery for melanomas in which the risk of recurrence is high. Interferon, interleukin-2, and Bacilli Calmette-Guerin are the most common biological therapy drugs used for melanoma.
Within each category are a number of treatments and medications. Your doctor will determine the best course of therapy based on your age, stage of melanoma, and other important factors. However, as with any therapy, it is best to understand the treatment you are receiving. Don’t be afraid to ask your doctor any questions you may have.
In addition, researchers are continually exploring new ways to treat melanoma. Some may be conducting research studies known as clinical trials, which test new medications and treatments that are being developed. (For example, a recent study showed that the biological agent ipilimumab nearly doubled the number of patients with advanced cancer surviving for one year.)
*All information on medical treatments on this site is provided as an overview only. For a complete and up-to-date list of side effects, warnings and precautions, read the product’s package insert and consult your doctor or a pharmacist.
**If you are considering an alternative or complementary therapy, discuss it with your doctor first, and always be sure to keep your doctor up to date about any vitamins, supplements, or other forms of alternative treatment you are taking. Like any medication, alternative therapies can interact with other medications/treatments and, in some cases, have side effects of their own. Remember that “natural” does not necessarily mean “safe.”
Coping and Support
A diagnosis of melanoma can deeply affect a person’s physical and emotional well-being. The condition is more likely to be fatal than other skin cancers and may return, even after intensive treatments such as surgery, chemotherapy and radiation. People who have been treated for melanoma can be left with scars after their cancer is removed or require reconstructive surgery. In addition, chemotherapy and radiation have short- and long-term physical side effects that can be difficult to manage.
For this reason, people with skin cancer who experience anxiety, depression or stress should get professional counselling to deal with their feelings or seek support from people who understand their situation
Resources
If you are living with Melanoma, or know someone who is, you may want to stay up-to-date on the condition as well as current treatments and news.
Our Affiliate Members:
![]() Canadian Skin Cancer Foundation
Canadian Skin Cancer Foundation

Other Resources
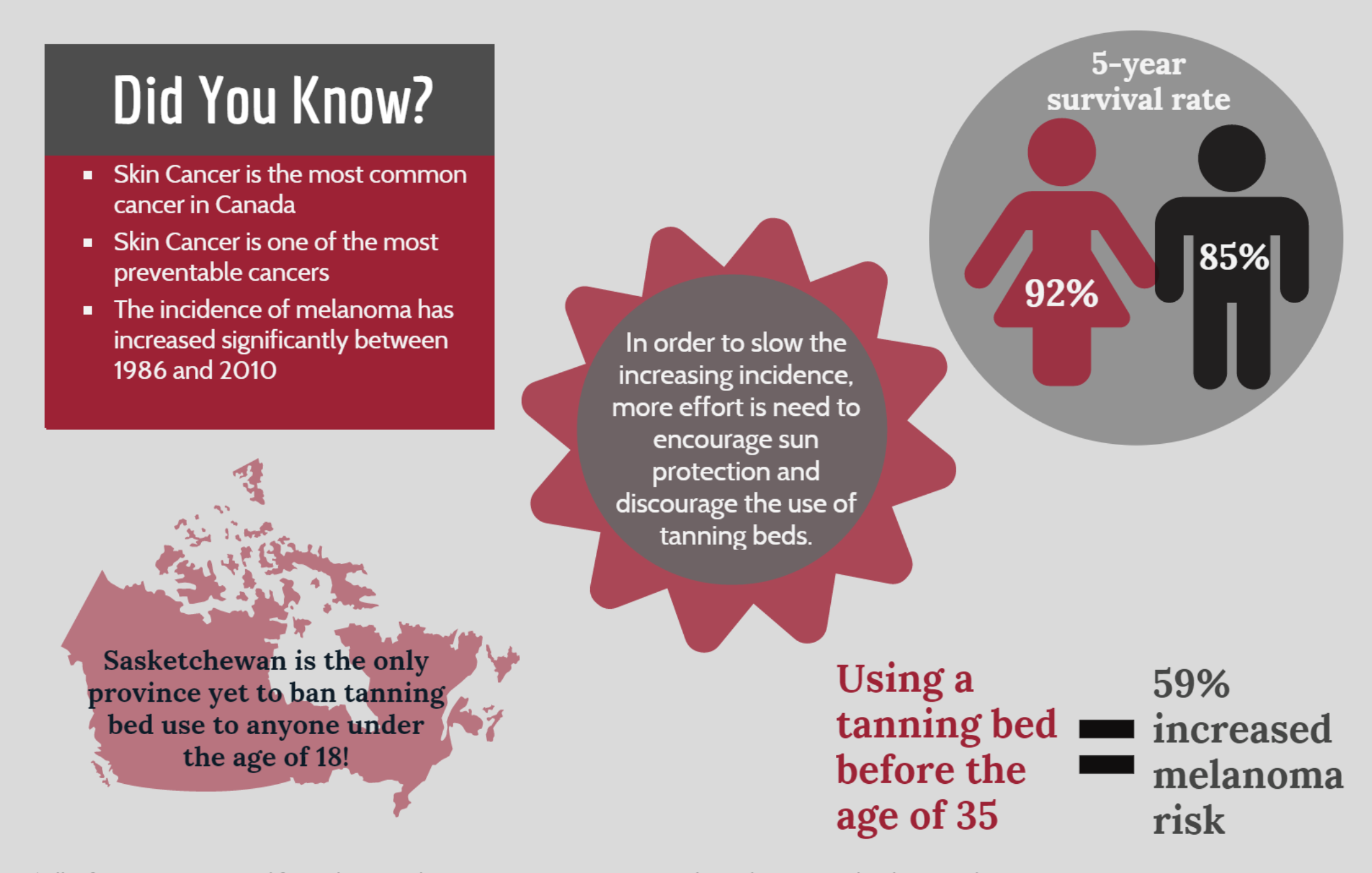
Melanoma Infographic
Cancer: Non-melanoma
Overview: What is skin cancer?
The information in this section has been gathered from existing peer-reviewed and other literature and has been reviewed by expert dermatologists on the CSPA Medical Advisory Board.
Skin cancer results from cells that multiply out of control. As a result, tumours, lumps, or masses can sometimes form on normal skin, and can be either benign (non-cancerous) or malignant (cancerous). Skin cancers are generally categorized as non-melanoma skin cancers (basal cell and squamous cell cancers) and melanoma.
There are three main types of skin cancer found in the outermost layer of skin, the epidermis:
- Basal cell carcinoma (least serious and most common)
- Squamous cell carcinoma (more serious than basal cell carcinoma, but less common)
- Melanoma (most serious and least common)
The difference among the three is the type of cells that the cancer affects. In the case of non-melanoma skin cancers (i.e., basal cell carcinoma and squamous cell carcinoma), the cell affected is the keratinocyte. In human skin, this cell starts out at the basal layer (the lowest layer of the epidermis) and then moves up to the squamous (or middle ) layer of our skin. The non-melanoma cancers derive their names from where in the epidermis the affected keratinocyte is located.
Keratinocytes are the most common cell in the epidermis, the outermost layer of skin. These cells produce keratin, a tough, highly fibrous protein that acts as a barrier in our skin to provide waterproofing and prevent injury and invasion from microbes. This protein is also found in our hair, nails and tooth enamel.
You are more likely to develop a non-melanoma cancer if you have a family history of skin cancer, have already had skin cancer, or have fair or freckled skin, blue eyes and light-coloured or reddish hair. However, anyone who has had excessive sun exposure, severe and frequent sunburns during childhood, or lives in a sunny or high-altitude climate is at increased risk of developing skin cancer. Those who use immunosuppression drugs following an organ transplant, and other patients with suppressed or weakened immune systems are also at higher risk of non-melanoma cancer.
Although you can’t change some of these risk factors, some ways to reduce your risk include decreasing sun exposure, using sunscreen or long-sleeved clothing, avoiding sunburns, having regular skin check-ups, and avoiding tanning lamps and beds.
Looking Deeper
One of the primary causes of the DNA damage that leads to skin cancer is exposure to ultraviolet (UV) radiation from the sun and tanning lamps. However, genetic predisposition also plays a part. In fact, researchers have identified several genes that are linked to skin cancer. The "patched" (PTCH) gene often changes in basal cell carcinomas, while the p53 gene sometimes mutates in squamous cell cancers. While likely not the only genes associated with these carcinomas, they do give researchers some new clues in understanding these diseases.
Causes
Basal cell carcinoma: Most basal cell carcinomas are caused by exposing unprotected skin to the ultraviolet (UV) radiation in sunlight. The UV radiation damages genes that regulate cell growth and division. One gene commonly found to mutate (change) in basal cell cancers is the “patched” (PTCH) gene. Changes in this tumour-suppressor gene, which normally helps keep cell growth in check, can allow cells to grow uncontrollably. PTCH is unlikely to be the only gene that plays a role in the development of this skin cancer. Researchers are still working to fully understand the cause.
Nevoid basal cell carcinoma syndrome: This rare genetic condition is also known as Gorlin syndrome, or basal cell nevus syndrome. It is characterized by numerous basal cell carcinomas of the skin as well as jaw cysts seen on xray, palmar and plantar pits, calcified folds of the brain seen by radiography, hamartomas, various noncancerous growths, and skeletal anomalies affecting the ribs, hands and face. Annual magnetic resonance imaging (MRI) for infants and children with the syndrome for medulloblastoma screening should be performed until the age of eight years.
Squamous cell carcinomas: Most squamous cell carcinoma is caused by exposure of unprotected skin to ultraviolet (UV) radiation. Repeated, unprotected exposure to UV light, especially in the few years previous to diagnosis, increases the risk of developing squamous cell carcinoma. The UV radiation damages genes that regulate cell growth and division. People with weak immune systems are also at greater risk of developing squamous cell cancers. The gene commonly found to mutate in squamous cell cancers is called p53. Changes in this gene, which normally causes cells to die, may cause abnormal cells to live longer and perhaps become cancerous. Gene p53 is unlikely to be the only factor in the development of skin cancer. Researchers are still working to fully understand the cause.
Actinic keratosis (AK): This condition consists of one or more pre-cancerous skin lesions (pre-malignant). Thought not a cancer, some researchers believe it is an early form of squamous cell carcinoma. Only a small percentage of actinic keratoses go on to become squamous cell carcinoma. The lesions are strongly associated with UV exposure and sun damage. (The words literally mean “sun-induced rough spots.”) Risk factors include being over the age of 40, exposure to high levels of UV radiation, and a weak immune system.
 Melanoma
Melanoma  Basal Cell Carcinoma Squamous Cell Carcinoma
Basal Cell Carcinoma Squamous Cell Carcinoma  Melanoma
Melanoma
Fast Facts
- Non-melanoma cancer statistics are not well documented since many cases are successfully treated in a doctor’s office and are not reported. In fact, most provincial cancer registries do not require doctors to count non-melanoma cancers.
- When reported together, basal cell and squamous carcinoma are classified as “non-melanoma cancers.”
- Basal cell carcinoma comprises 80 per cent of non-melanoma cancers.
- Basal cell carcinoma can recur in the same or other places on the skin. Within 5 years of diagnosis, 35-50 per cent of patients develop a new skin cancer.
- Squamous cell carcinoma comprises 20 per cent of non-melanoma cancers.
- Actinic keratosis is one of the most commonly treated conditions by dermatologists.
- Only a small percentage of cases of Actinic Keratoses can become skin cancer. Some cases go away on their own.
- In Canada, 74,100 new cases of non-melanoma cancers are estimated for this year; of these, 264 will likely be fatal.
- In the United States, approximately 1 million cases of non-melanoma cancer are diagnosed each year; of these, about 2000 result in death.
Symptoms
The most common sign of skin cancer is a local change in the skin’s colour or a sore that does not heal. However, skin cancer symptoms vary widely according to type, so it’s wise to check your skin regularly to catch any potentially cancerous marks early.
Basal Cell Carcinoma
This type of cancer begins in the lowest layer of the epidermis (the basal cell layer), usually on sun-exposed areas, such as the head, neck, and upper shoulders. However, 20% of people with basal cell carcinoma develop it in areas not exposed to the sun. This type of cancer grows slowly and rarely spreads to other parts of the body, but if left untreated, it will continue to grow and may ultimately invade the bone or other tissues beneath the skin. Basal cell carcinoma is usually treated successfully as an out-patient procedure. Symptoms include:
- A small, dome-shaped bump, frequently covered by small, superficial blood vessels
- A bump that is pearlescent, shiny or translucent
- May become scaly or crusty patches or open sores with a pearlescent or milky appearance and raised edges
- Bleeding after minor injury
- Growths enlarge may very slowly so subtle changes may not be noticed
Nevoid basal cell carcinoma syndrome
Skin growths are similar to basal cell carcinomas. In addition, the person may also have:
- Hamartomas (e.g. retinal) - overgrowth of normal cells
- Medulloblastomas - a low grade tumor of the brain
- Meningiomas - localized benign growth of the cells lining the brain
- Calcified ovarian fibromas - benign ovarian fibrous growth
- Cardiac fibroma - non cancerous fibrous growth of the heart
Squamous Cell Carcinoma
This carcinoma begins in the upper layer of the epidermis (squamous cell layer), usually on sun-exposed areas, such as the head, neck and back of the hands. However, it may appear on skin elsewhere on the body (such as the lips, tongue or the lining of the mouth) and on skin that has been burned or exposed to chemicals or radiation therapy. Of these tumours, 95 per cent can be cured if found and treated early, particularly if they arise in areas of sun-damaged skin. Rarely, squamous cell carcinomas can grow and spread to lymph nodes. Symptoms include:
- Firm, red bump
- Scaly, bleeding or crusty growth or patch of skin
- Sore that does not heal
- As it grows, it may become raised and firm
- Eventually, it may appear like an open sore (not always) and grows into the underlying tissue
Bowen’s disease isatype of squamous cell carcinoma limited to the epidermis. The affected area is red-brown and scaly or crusted and flat. It may resemble a patch of dermatitis, psoriasis, a fungal infection or a type of basal cell carcinoma.
Actinic Keratosis
These spots can look like regular skin, but may feel like sandpaper. Symptoms and signs include:
- Barely visible spots or localized red areas of skin
- May become thick, scaly and sometimes crusty patches of skin
- May change to a yellow-brown colour
- Visible spots may range between a few millimetres up to 2 cm or more in diameter.
- Skin discoloration, which may include dark or light pink, red skin
Treatment
To diagnose non-melanoma carcinomas, a doctor will take your medical history and perform a physical exam. If cancer is suspected, your doctor may take a skin biopsy, which will be used to confirm the diagnosis. A biopsy can be taken in one of four ways:
- The entire growth is removed.
- A sample of the area of concern is removed because the tumour goes into deeper layers of the skin. This technique is called “Shave and Punch”
- A “shave and punch” biopsy takes a sample through multiple skin layers.
A biopsy can be done in the doctor’s office or in a hospital’s outpatient department. It requires a local anesthetic and sometimes stitches, depending on how much skin is removed. The tissue sample will then be checked with a microscope to determine the diagnosis. .
Generally, the earlier non-melanoma skin cancers are caught, the more successfully they can be treated. Visit your doctor if you develop a new skin lesion that does not heal, notice a change in a pre-existing skin lesion (such as a mole), or have any of the symptoms or signs of non-melanoma carcinoma.
Treatment
Basal cell carcinoma treatments include the following:
- Surgery is often the primary treatment for basal cell carcinoma, and there are several different methods that can be used. An excision removes the tumour and surrounding skin. Curettage and electrodessication involves scraping the tumour from the skin and using an electric current to destroy any remaining tumour cells. Mohs surgery is a specialized technique that removes the visible tumour as well as an additional layer of tissue around the tumour. This layer of tissue is examined with a microscope to identify any remaining cancer cells. If this layer of tissue contains cancer cells the process is repeated until no tumour cells remain. Lymph node removal is not usually required for basal cell carcinoma.
- Radiation therapy uses high energy rays or particles to kill cancer cells. It is primarily used for older people who cannot tolerate surgery. It is not the preferred treatment for younger patients because radiation may cause long-term damage. In external beam radiation therapy, a machine directs radiation to the tumour and surrounding area. Radiation therapy is often used for tumours on the ear, eyelid, lip and nose because it doesn’t remove normal tissue like surgery does. Topical drugs are most commonly used in chemotherapy for basal cell carcinoma. Topical 5-fluorouracil (5-FU) cream is applied directly to the tumour for several weeks or injected directly into the tumour. Only superficial tumours are treated this way as treatment does not reach tumours in the deeper layers of skin.
- Systemic drug treatments are rarely used for basal cell carcinoma. When they are used, the most common systemic agent injected intravenously is cisplatin.
- Biological therapy (immunotherapy) uses natural or manufactured agents to strengthen the immune system. Biological therapy is used only on low-risk, superficial basal cell carcinoma. Imiquimod is the most common biological drug used to treat basal cell carcinoma.
Nevoid basal cell carcinoma syndrome can be treated through:
- Surgery
- Photodynamic therapy has been used in some cases
Squamous cell carcinoma treatments include:
- Surgery
- Radiation therapy
- Chemotherapy
- Systemic drug treatments for squamous cell carcinoma are injected intravenously and include cisplatin, 5-FU, doxorubicin and mitomycin.
Actinic keratosis treatments involve:
- Lesion-directed: removal of a single or multiple skin lesions using procedures such as cryotherapy (freezing)
- Field-directed: treatment of an area of skin affected by AK through the application of topical creams or gels, or using photodynamic therapy
In addition to the treatments above, Canadian researchers are continually exploring new ways to treat non-melanoma skin cancers. Some may be conducting research studies known as clinical trials, which test new medications and treatments that are being developed. To learn about new research on all types of non-melanoma cancers happening in Canada, visit the clinical trials section [link to clinical trials section].
Footnote
*All information on medical treatments on this site is provided as an overview only. For a complete and up-to-date list of side effects, warnings and precautions, read the product’s package insert and consult your doctor or a pharmacist.
**If you are considering an alternative or complementary therapy, discuss it with your doctor first, and always be sure to keep your doctor up to date about any vitamins, supplements, or otherCoping and Support
Although a cancer diagnosis is never welcome news, basal cell carcinomas are usually easily curable. With such high success rates, they usually do not negatively impact a person’s everyday life. However, patients may feel anxious knowing that their cancer may return, or may feel depressed if surgical removal of larger tumours leaves a scar or causes extensive damage to underlying tissues or bone.
Most squamous cell carcinomas are also easily treated and generally do not affect a person’s quality of life. In rare instances, people with this disease may suffer emotional trauma if their cancer progresses and requires long-term treatment or becomes life-threatening.
Non-melanoma skin cancers are curable most of the time, especially if caught early. With this, gentle reassurance alone is often sufficient to help someone successfully manage their fears. However, people with skin cancer who experience anxiety, depression or stress may seek professional counselling to manage their feelings or seek support from others who understand their situation.
Resources
If you are living with Skin Cancer, or know someone who is, you may want to stay up-to-date on the condition as well as current treatments and news.
Our Affiliate Members:
![]()
Canadian Skin Cancer Foundation
Other Resources
Chronic Idiopathic Urticaria
Overview: What is CIU?
Overview: What is Chronic Spontaneous Urticaria (CSU)?
Symptoms
Hives are itchy, transient and of various sizes. These appear as red, white, or flesh-colored bumps with distinct edges that may change shape. Your doctor may call them "wheals." Wheals can be as small as a pencil tip or larger. The itch cause by hives can be mild to severe.
Hives can show up anywhere on the body. They may also "move around." For instance, they may appear on your hand, go away within a day and then show up on your shoulder. Hives often occur on the chest, back, arms, and legs.
A red hive will turn pale when pressed in the center. This is called "blanching.”
The discomfort caused by hives can result in sleep deprivation. Social isolation, anxiety and depression are also common due to CSU.
Angiodema is another symptom experienced by some patients. This is severe swelling, particularly on the eyelids, lips, genitals, tongue, hands and feet. 15% of patients will experience just this swelling and not the hives.
Treatment
Diagnosis
Dermatologists and allergists can both diagnose CSU based on the following information:
Blood test - A blood sample may be taken to count the different parts of your blood, like white blood cells and red blood cells. This may be done to rule out infection as the cause of your hives.
Skin test - Your skin may be pricked to confirm whether you have allergies.
These tests and more may be done to rule out any other health conditions that could be causing your symptoms.
If a cause still isn't found, your doctor may diagnose you with CSU.
Treatment
Antihistamines are generally the first treatment option.
An injectable medication can also be prescribed, that is currently used to treat adults and children 12 years and older with CSU
To help with the itch and swelling, an oral steroid may also be prescribed to you for short periods of time.
Coping and Support
First and foremost – stay cool, stay calm
• Keep your skin cool. Stay in air-conditioned environments for as long as possible in summer.
• Do your best to reduce stress. Consider taking up a relaxing hobby or activity, like yoga or meditation. Ensure you get enough sleep.
Take care of yourself and your surroundings.
- Pamper yourself!
- Apply cool, wet compresses to your skin. Covering the affected skin with bandages
or dressings can be soothing and also prevent scratching. - Take a cool bath. But not too cold – make it comfortable! Adding some baking
soda, uncooked oatmeal or colloidal oatmeal to help with itching. - Dress for success! Wear loose, smooth-textured clothing, preferably cotton. Avoid tight, scratchy, or rough material, including wool.
- Avoid anything that aggravates your CIU, irritates your skin or causes an allergic reaction. This includes certain foods like spicy food, medications, pollen, pet dander, scented household cleaning products, latex or insect stings.
- Cut down on the drinking! Alcohol consumption may aggravate symptoms.
Track your symptoms and keep a diary of when and where the hives start, when you experience a worsening of symptoms and what you ate that day.
Resources
Many people with CSU—whether they seek treatment or not—may want to stay up-to-date on the condition as well as current treatments and news. The following websites are valuable sources of information:
Our Affiliate Member
Canadian Chronic Urticaria Society
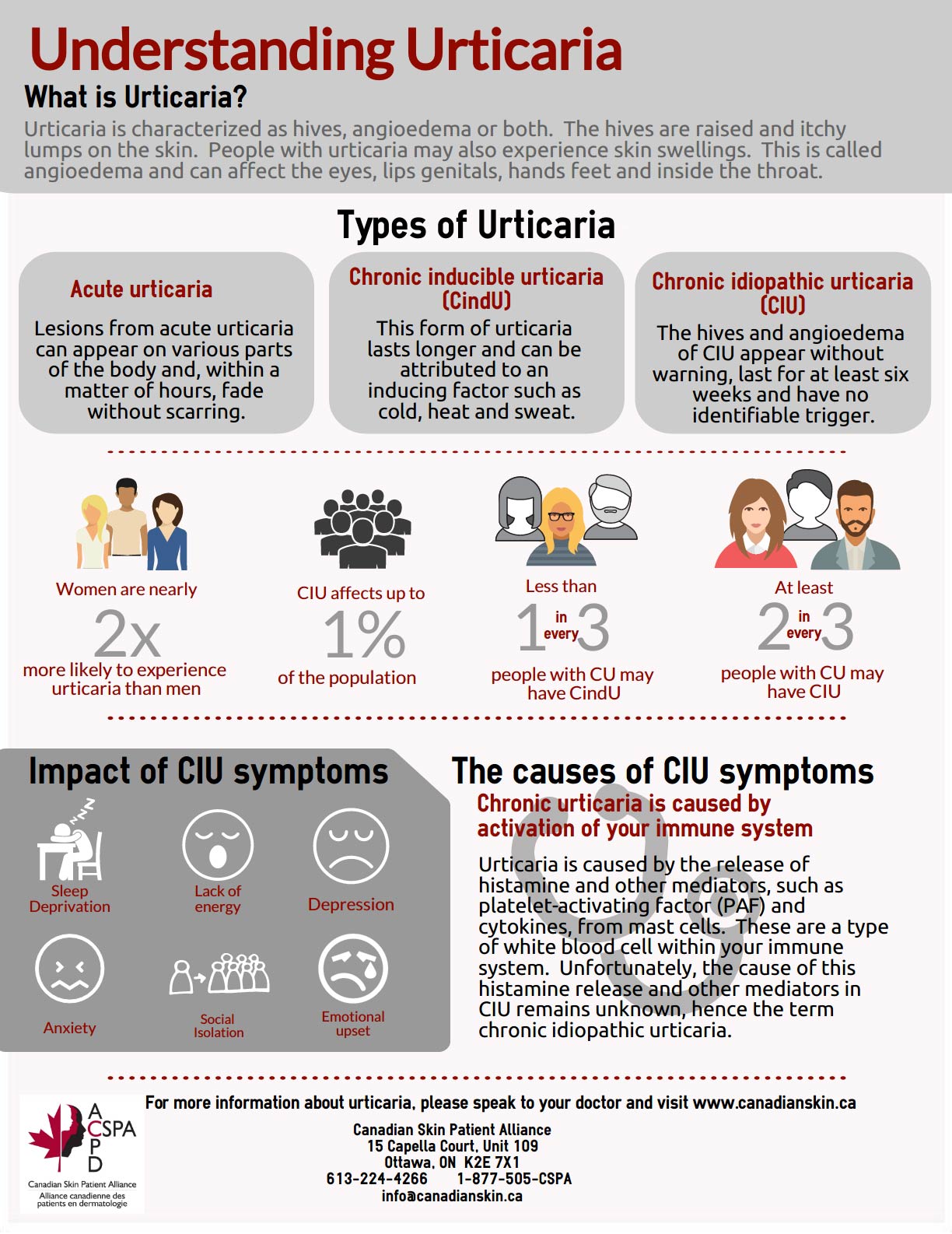
CSU Infographic
Cold Sores
Overview: What are Cold Sores?
Cold sores, also called Herpes Simplex Labialis (HSL), are a fact of life for millions of Canadians. They are caused by the Herpes Simplex Virus (HSV). The cold sore is the body's visible reaction to the Herpes Simplex Virus and appears as clusters of small blisters on the lips, around the mouth (especially the corners), and occasionally inside the nose. The virus is highly contagious and can be transmitted through contact, such as kissing, sharing utensils or towels, not only during an outbreak but also when no symptoms are present.
Fast Facts
• It is estimated that cold sores affect one in five Canadians annually
• Without treatment cold sores typically heal within 10-21 days
• Cold sores have a rate of frequency that varies from rare episodes to 12 or more recurrences per year.
• There is currently no cure for the Herpes Simplex Virus
• The herpes virus can be transmitted even when patients have no visible symptoms through direct contact
• There are rumors that home remedies such as applying a tea bag, an ice cube or alcohol on the affected area could prevent cold sores or speed up the healing time. None of these techniques have been proven to be effective.


Symptoms
Symptoms of Cold Sore Outbreaks
Cold sore outbreaks can be caused by a variety of triggers including:
- emotional and physical stress,
- colds or other upper respiratory tract infections,
- hormone changes (i.e. menstruation),
- sun or wind exposure without protection
- local trauma or injury to the skin around the lips (i.e. dry cracked lips, cosmetic surgery, chemical peels, or laser therapy).
In advance of a cold sore break out, sufferers often report fatigue, redness, tingling or burning sensation, and/or itching or pain around their lips or mouth. This is known as the prodromal stage, which is followed by the blister stage (where inflammation and the eruption of the blisters occur).
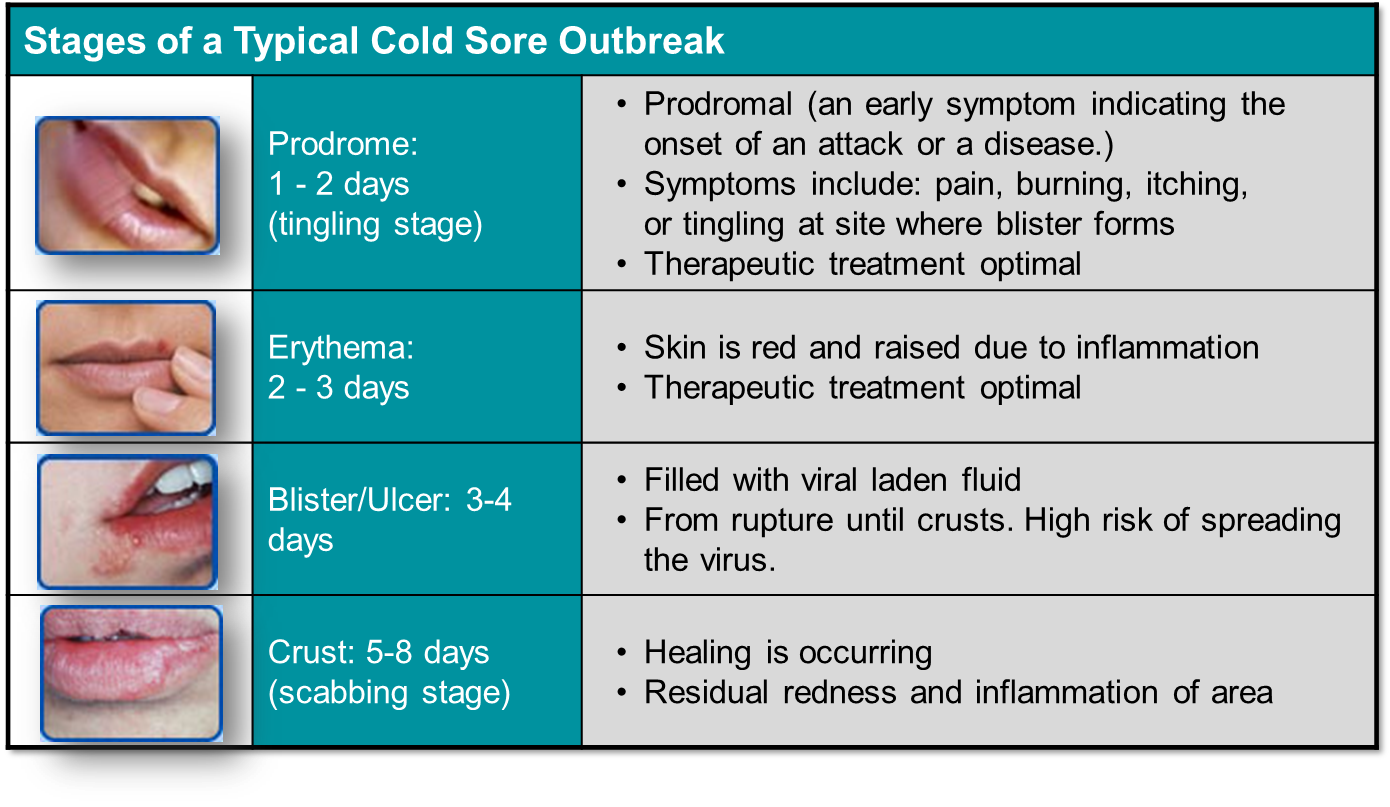
Treatment
The diagnosis of Herpes Simplex Labialis is often recognized by the clinical appearance alone. If a lesion is atypical, laboratory investigations can be ordered by your physician that will identify HSV-1, HSV-2, or will return a negative result. The best way to minimize the impact of a cold sore is to treat it at the first sign of symptoms (tingling, burning, and itching).
Currently available treatments include prescription and non-prescription drugs in topical and oral formulations, with antiviral medication representing a mainstay of treatment. A new formulation in the form of a cream has recently been approved by Health Canada and combines an antiviral agent and an anti-inflammatory agent, making it the only treatment to reduce viral shedding and inflammation.
The most effective way to seek treatment for your cold sores is to consult a doctor. Your physician can recommend an over-the-counter medication to minimize symptoms or a prescription cream or oral medications that are proven to help prevent cold sore outbreaks and speed up the healing time.
Tell your doctor how many cold sores you typically suffer from in one year and how long do they usually last. Also, speak to your doctor about the impact of cold sores on your quality of life. This will help your doctor to guide you to the best available treatment. Tip: Once you find the treatment that works for you, ask your doctor for many prescription repeats that you can leave with your pharmacist in order to access the prescription medication at the first sign of a cold sore.
Non-prescription treatments:
Viral Entry Blocking Agent Docosanol (Abreva)
This is non-prescription medication (over the counter). Abreva has been proven to reduce the symptoms and the length of the cold sore outbreak. This agent has not been proven to help stop cold sore progression. Abreva is most effective if used at the first sign or symptom of a cold sore.
Skin Protectants and Analgesics
- Skin protectants and lip moisturizers with allantoin, dimethicone, cocoa butter, white petrolatum, or glycerin provide moisturization to keep the cold sore moist as well as a mechanical barrier to guard the skin and lips against irritants
- Topical analgesics/anaesthetics including benzocaine, lidocaine, benzyl alcohol, camphor, menthol, and phenol help provide local pain control and may help reduce the itching
- Oral analgesics such as ibuprofen and acetaminophen also provide temporary relief from the pain
Prescription treatments
Topical treatment (creams and ointments)
Combination Antiviral and anti-inflammatory agent (Xerese)
This agent is available in a cream format and combines an antiviral (acyclovir 5%) and an anti-inflammatory (hydrocortisone 1%) agent. XereseTM works in two ways. It reduces viral shedding and it reduces inflammation. Xerese has been proven to help prevent cold sore progression. It is also proven to decrease the size of the lesion and speed up the healing time. For optimal results it should be used at the first sign of a cold sore.
Systemic treatments
Oral Antivirals
Oral antivirals (such as Valtrex, Famvir, Zovirax) may help to prevent a cold sore from ulcerating and shorten the healing time if taken at the prodromal stage. Systemic antivirals are oral medications that act on reducing viral shedding. For optimal results, it should be used at the first sign of a cold sore.
Coping and Support
In addition to the pain and tenderness that occur before and during a breakout, cold sores profoundly affect quality of life. According to a recent survey, 50 percent of respondents identified that cold sores gave them a negative self-image and limited their social lives. In fact, many Canadians who suffer from cold sores are afraid to tell others about having the virus, including friends, family and sexual partners. Further, outbreaks often influence quality of life due to embarrassment and have been linked with depression, fear of rejection and isolation.
People with cold sores must also take precautions:
- Never touch an open sore and then your eye, as it can result in herpes keratitis.
- Avoid touching the open sore and other areas of your body including other areas of the lips
- Avoid touching a new-born baby, as newborns can be infected by exposure to HSV, the virus that causes cold sores
- Use condoms or other barriers during oral sex to reduce the risk of transmission.
The pain and discomfort related to cold sores are best managed with the help of your doctor.
Connective Tissue Disorder
Overview: What is Connective Tissue Disorder?
The information in this section has been gathered from existing peer-reviewed and other literature and has been reviewed by expert dermatologists on the CSPA Medical Advisory Board.
A connective tissue disorder targets the body’s connective tissues, which are the structural materials (mainly the proteins, collagen and elastin) that hold the cells of the body together. With a connective tissue disease, these proteins are injured by inflammation and can affect the skin, joints, bones, heart, blood vessels, lungs, eyes, and ears.
Connective tissue disorders that directly affect the skin include the following:
Lupus erythematosus is an autoimmune disease, meaning the immune system mistakenly attacks parts of the body it normally protects. In lupus, this leads to inflammation and damage to various tissues, including skin, joints, kidneys, heart, lungs, brain and blood vessels. When only the skin is affected, the condition is called discoid lupus (DLE) or subacute cutaneous lupus (SCLE). When internal organs as well as skin are affected, the condition is called systemic lupus erythematosus (SLE).
The cause of lupus erythematosus is unknown. Viruses, ultraviolet light and some drugs may trigger the immune system to attack its own tissues. Female hormones may also influence the appearance of lupus erythematosis. Recently, research has led scientists to suspect that a mutation in a gene responsible for the disposal of dying cells may be involved in triggering the disease. There is currently no cure for lupus, but it is effectively treated with drugs, allowing people to live active and healthy lives.
Rheumatoid arthritis (RA) is a chronic autoimmune disease that causes pain, swelling, stiffness and loss of function in the joints. The wrist and finger joints are commonly affected, but the knees and other body parts may also be involved. Frequent flare-ups may result in long-term joint damage, resulting in chronic pain, loss of function and disability.
The skin may also be involved. Small nodules sometimes appear just under the skin, usually on a bony area near an affected joint. Dark areas, caused by blood seeping from damaged blood vessels, skin rashes and lesions—all due to vasculitis (inflammation of the small blood vessels)—are also seen in some people with RA.
There is no cure for rheumatoid arthritis, but it can be controlled through a combination of drugs, exercise and joint protection techniques.
Scleroderma is a chronic autoimmune disease in which the skin hardens and thickens. There are two major classifications of scleroderma: localized, or morphea, which affects the skin only, and systemic, which affects the blood vessels and internal organs. Symptoms may be mild or severe. As the disease progresses, some people may be unable to carry out everyday tasks. Complications of systemic scleroderma may lead to serious problems with the body’s major organs, such as the lungs. People with systemic scleroderma should have lung function checked periodically.
Scleroderma results from overproduction and accumulation of collagen, a fibrous protein that makes up the connective tissues in the body. Accumulation of collagen in the skin results in the thick, hard layers characteristic of scleroderma. In systemic scleroderma, this process also affects other organs of the body. The trigger for abnormal collagen production remains unclear, but researchers believe the immune system plays a key role. There is no cure for scleroderma, but treatment can relieve its symptoms.
Dermatomyositis is a disease characterized by muscle weakness and a distinctive bluish-purple or reddish skin rash on various parts of the body. It may occur at any age but tends to affect adults between 40 and 60 years of age and children between 5 and 15. During periods of remission, symptoms spontaneously improve.
The cause of dermatomyositis is unknown, however, researchers suspect that it is an autoimmune disorder. Genetics may also play a role. The person’s immune system is triggered to attack the blood vessels supplying oxygen to muscle and skin. The exact triggers have not been identified, but some researchers believe that exposure to certain drugs or viruses may play a role. Sometimes it can be associated with an internal cancer, so adults with this condition should be checked to rule this out. There is no cure for dermatomyositis, but the symptoms can be treated.
 Lupus
Lupus  Scleroderma
Scleroderma  Lupus 2
Lupus 2
Symptoms
Lupus Erythematosus
Symptoms vary from person to person and may come and go. Some symptoms are more common than others and may be mild or severe. Common symptoms include:
- Painful or swollen joints
- Muscle pain
- Fever
- Red “butterfly” rash over nose and cheeks
- Chest pain upon deep breathing
- Unusual loss of hair
- Pale or purple fingers or toes from cold or stress (Raynaud’s phenomenon)
- Sun sensitivity
- Swelling (edema) in legs or feet; weight gain
- Seizures or psychosis
- Mouth ulcers
- Swollen glands
- Extreme fatigue
The type and severity of symptoms depend on the areas of the body that are affected. In discoid lupus, a rash is typically the only symptom. The rash does not usually itch or hurt, but it may scar. In systemic lupus erythematosus, many body systems are involved. Additional symptoms may be present that are related to inflammation in these areas.
Rheumatoid Arthritis
The major symptom is joint pain. Other symptoms include:
- Pain and swelling in the joints, especially of the wrist and hand
- Pain and swelling that is symmetrical (e.g., in the same joints on both sides of the body)
- Stiffness after long periods of sitting or in the morning
- Possible inflammation in other body tissues or organs
- In some people, lumps (rheumatoid nodules) under the skin, often over bony areas
- In some people, dry eyes and mouth
- Flu-like symptoms (fatigue, weakness, low fever)
- Muscle pain
- Loss of appetite, weight loss, depression
- Cold or sweaty hands and feet
The symptoms, which vary among individuals, may start gradually or with a sudden attack. In some people, the disease is characterized by mild flare-ups with periods of inactivity. In other people, the disease is continuously active and may progress over time.
Scleroderma
Localized scleroderma affects only the skin and the deep tissues below the skin. Systemic scleroderma affects not only the skin but the blood vessels and internal organs. The progression of scleroderma varies widely. Disease that involves major organs such as the lungs, heart or kidney can lead to severe disability or death if left untreated. Symptoms include:
- Shiny, thick, hard areas of skin
- Numbness, pain, or colour changes in fingers or toes from cold or stress (Raynaud’s phenomenon)
- Stiff, painful joints
- Curling of the fingers
- Patches of enlarged blood vessels on the skin
- Digestive problems (acid reflux, difficulty swallowing, bloating)
- Sores over joints
- Puffy hands and feet, particularly in the morning
Dermatomyositis
The major symptoms are a distinctive rash and progressive muscle weakness. Other symptoms may include:
- Red or violet, hardened or scaly skin rash most commonly on the face, eyelids, neck, chest, and overlying joints such as the knuckles, knees and elbows. Affected areas may be sensitive to sun.
- Muscle weakness, particularly in the hips, thighs, shoulders, upper arms and neck. This weakness is symmetrical, appearing on both sides of the body.
- Muscle pain
- Tiredness, fever and weight loss
- Difficulty swallowing (dysphagia)
- Hardened deposits of calcium under the skin (calcinosis), especially in children
- Gastrointestinal ulcers and infections, especially in children
- Lung problems (weakness of muscles used for breathing, fibrosis, coughing, shortness of breath)
Treatment
Each connective tissue disease is diagnosed based on particular symptoms, a thorough physical examination, and the results of lab tests, including blood work. In some cases, the symptoms of one disease can overlap with those of another so much so that it is difficult to distinguish between them. In this situation, a doctor may make a diagnosis of overlap disease or undifferentiated connective tissue disease. When a disease affects a specific organ or tissue, a doctor may also perform a biopsy. The results from this test, which involves removing tissue and looking at it under a microscope, can be used to either confirm a diagnosis or monitor the disease’s progression.
Treatment for connective tissue diseases is unique to the specific condition.
Lupus Erythematosus
Treatment is directed at controlling symptoms and preventing flare-ups. (Note that people may be sensitive to sunlight; sunscreen should be worn to prevent flare-ups.) Treatment plans are personalized to meet each person’s needs. Someone with a mild form may require no treatment at all. Treatment plans include:
Medication
The type of medications depend on the organs affected and extent of symptoms. One or more of the following may be prescribed:
- Acetominophen to manage pain
- Nonsteroidal anti-inflammatory drugs (NSAIDS) to reduce inflammation
- Oral cortisone to reduce inflammation and control the immune system
- Antimalarial medication to reduce fatigue, rashes and joint pain
- Cytotoxic drugs to control inflammation and suppress the immune system
Diet
- Alcohol and smoking may trigger inflammation and lead to flare-ups.
- An unbalanced diet may contribute to flare-ups.
Exercise
- Regular exercise may help manage pain and stress.
- Medical professionals can design an exercise program to reduce stiffness, increase muscle strength, strengthen the heart, and control weight and energy levels.
Rheumatoid Arthritis
Controlling symptoms and preventing flare-ups are the goals of treatment. Each plan is customized to meet the needs of each person. Early treatment is essential to minimize the risk of disability and/or deformity. Treatment plans include:
Medication
One or more of the following may be prescribed:
- Nonsteroidal anti-inflammatory drugs (NSAIDS) to reduce inflammation and pain
- Disease-modifying anti-rheumatic drugs (DMARDS) to slow down or prevent immune attack of the joints
- Corticosteroids to reduce swelling
- Biologic response modifiers to block specific hormones involved in inflammation
Exercise
- Regular exercise may help manage pain and stress.
- Medical professionals can design an exercise program to reduce stiffness, prevent further joint damage, increase muscle strength, strengthen the heart, and control weight and energy levels.
Application of heat/cold
- Heat may relax aching muscles and reduce joint pain.
- Cold may reduce pain and swelling.
Surgery
People whose disease does not respond to other treatments may consider surgery. Surgical procedures may be used to
- clean out damaged joint tissue
- realign joints
- fuse joints
- rebuild parts
- replace joints
Scleroderma
Treatment, which is customized for each person, is directed at controlling symptoms. Treatment strategies include the following:
Medication
One or more medications may be prescribed. These include:
- Nonsteroidal anti-inflammatory drugs (NSAIDS) to reduce inflammation and pain and reduce stiffness
- Disease-modifying anti-rheumatic drugs (DMARDS) to slow down progression of the disease
- Oral cortisone to suppress inflammation and control the immune system
- Penicillamine to stop or slow over-production of collagen
- Depending on organs affected, medications to control specific problems may be used.
Exercise
- Exercise can be useful for improving blood flow in affected areas.
- Certain exercises can help maintain muscle strength and joint mobility.
Skin and body care
- The affected skin is prone to drying. Use of humidifiers in the home, baby oil in baths, and application of creams and lotions will help keep skin moist.
- To improve blood circulation in the affected areas, people with the condition should wear socks and gloves in cold weather and avoid smoking, which causes blood vessels to constrict.
- People with calcium deposits under the skin should avoid putting pressure on these areas, as the skin may break and become infected.
- Those whose scleroderma affects the esophagus may have trouble swallowing and should chew slowly. Eating smaller, more frequent meals will help decrease acid reflux.
Surgery
People with severely restricted blood flow to an area of the body may require surgery to reduce blood-vessel spasms that lead to poor circulation. Surgery may also be recommended to remove calcium deposits under the skin.
Dermatomyositis
Treatment is directed toward managing symptoms. Many people experience only a single attack and are able to stop treatment. Others may have several attacks that respond well to treatment. (Note that people may be sensitive to sunlight; sunscreen should be worn to prevent flare-ups.) Rarely, some people have chronically active disease and must continuously take immunosuppressive medications. Treatment plans include:
Medication
One or more medications may be prescribed. These include:
- Oral cortisone to reduce inflammation and regulate the immune system
- Disease-modifying anti-rheumatic drugs (DMARDS) to slow down progression of the disease
- Gamma globulin
Rest/Exercise
- When the disease is active, rest is recommended to prevent muscle strain.
- When the disease is inactive, exercise is recommended to keep muscles from weakening.
As research into many of these diseases is ongoing, people may want to stay abreast of new treatments or medications used to treat these conditions. Visit the Clinical Trials page [link to CSPA clinical trials page], to see if new forms of treatment are being tested.
Footnote:
*All information on medical treatments on this site is provided as an overview only. For a complete and up-to-date list of side effects, warnings and precautions, read the product’s package insert and consult your doctor or a pharmacist.
**If you are considering an alternative or complementary therapy, discuss it with your doctor first, and always be sure to keep your doctor up to date about any vitamins, supplements, or other forms of alternative treatment you are taking. Like any medication, alternative therapies can interact with other medications/treatments and, in some cases, have side effects of their own. Remember that “natural” does not necessarily mean “safe.”
Coping and Support
Connective tissue disorders can have potentially debilitating symptoms, particularly during periods where the disease is active, which may affect your ability to function in your day-to-day life. Some troublesome symptoms can include:
- In systemic lupus erythematosus, pain at multiple sites and extreme fatigue.
- Rheumatoid arthritis can lead to crippling joint deformities.
- Thickened skin leaves people with scleroderma with stiffness and loss of dexterity, making simple tasks like picking up a pencil difficult.
- Muscle weakness leaves people with dermatomyositis easily fatigued.
You can manage the physical impact of the symptoms of connective tissue disease by:
- Following your personal treatment plans to minimize symptoms and keep the disease under control.
- Practising techniques that protect the joints. For example,
- take breaks between heavy tasks to allow weak muscles to rest
- use devices such as canes and carts to take stress off the joints
- use aids such as grab bars and shower seats to avoid falls
- Practising relaxation techniques to relax muscles and reduce pain
In addition, you may experience feelings of helplessness, hopelessness or depression from knowing that these disorders are at present incurable. To manage the psychological impact of these disorders:
- Practise relaxation techniques to reduce stress and fatigue
- Obtain professional counselling to develop a positive outlook, manage stress, and gain a feeling of control
Dermatomyositis
Overview: What is Dermatomyositis?
Dermatomyositis (DM) is a condition that can cause muscle weakness and skin rashes. Both the skin and the muscles become inflamed in DM. Furthermore, a minority of individuals with DM will also develop lung problems. It is not certain as to what the cause of DM is, but it is believed that it is caused by an immune-mediated process triggered by outside factors (e.g. drugs, infectious agents) in genetically predisposed individuals. Adult women are affected twice as often as men yet in children it does not affect one sex over another. The incidence of DM is 2-7 per million individuals. The peak incidence of BM occurs in children 10-15 years and adults 45-47 years.
Symptoms
Muscle Weakness: Muscle weakness will affect the body in a symmetric fashion, and this typically occurs gradually over time. Muscles that tend to be affected are the neck, shoulders, hips and thighs. Patients will complain of general fatigue, lack of energy, and are typically unable to perform simple tasks such as climbing up the stairs, swallowing, or even lifting heavy objects. In more advanced stages of the disease, muscles can be tender when touched. Patients typically complain of muscle pain.
Skin Rashes: There are a variety of rashes that can develop in DM, on different parts of the body. The rashes are typically red, itchy, and sometimes covered in scales. Exposing the skin to sunlight can make the rash worse. Rashes are commonly seen on the: fingers (including the finger joints and around the fingernails), elbows, knees, upper eyelids, neck, upper chest, upper back, and scalp.
Interstitial Lung Disease: Approximately 15-30% of patients with DM, will develop interstitial lung disease. This causes inflammation and scarring of the lungs and can make it more difficult for oxygen from the air to enter the lungs. This makes it much more difficult to breathe.
Malignancy: The development of adult DM has been associated with cancer, as rates can vary from 10% to 50%. Some of the cancers that have been identified include: ovarian cancers, colon cancers, breast cancer, lung cancer, gastric cancer, pancreatic cancer, and lymphomas (non-Hodgkin) and others
Treatment
Diagnosis
The following tests can be ordered by your clinician in order to accurately diagnose DM.
- Blood Tests: Various muscle enzymes will be seen as elevated in patients with DM. There will also be a higher level of myoglobin (oxygen-binding protein found in muscle tissue). Moreover, there will be an increase in immune cells known as autoantibodies.
- Electromyography (EMG): AN EMG test can be used to assess if your muscles are responding to the electric nerve signals properly.
- Muscle Biopsy: Muscle biopsies will be taken typically from the deltoid (shoulder) or triceps.
- Skin Biopsy: A small biopsy of the skin should be removed and thus can be assessed under a microscope to confirm the clinical impression of DM.
- Magnetic Resonance Imaging (MRI) scan: An MRI scan can be performed to identify areas of muscle that are most inflamed.
Treatment
The primary treatment method for DM is to take oral steroids. Steroids, specifically prednisone, can help decrease inflammation, improve muscle strength and preserve muscle function. Patients will typically be on prednisone for approximately one year, with higher doses in the first several months and a slow taper between 9 and 12 months. The slow taper is important as prednisone can cause your own body to produce less adrenal steroid.
If you cannot take steroids, or if the steroids are not helping enough, there are other medications available to take. These medications help to relax the immune system. The drugs of choice are azathioprine or methotrexate.
Itchiness is a common complaint of patients with DM. Your physician can provide you with a topical or oral medication to help decrease this sensation.
As mentioned previously, because the skin rash is very sensitive to light, it is important that patients use sunscreen liberally and have on sun-protective clothing (e.g., long-sleeved shirt, long pants, wide-brimmed hat). Also, medications should be taken to prevent the side effects of steroids.
If a patient is having difficulty eating, due to difficulty with swallowing or choking readily on food, several interventions can help reduce this issue including speech therapy advice, elevating the head of the bed, and semi-thick diets. A gastric feeding tube may be necessary to help protect the airways for some patients. Exercise and physical therapy should begin early in the treatment plan to maintain muscle strength.
Coping and Support
The severity of DM is very individual dependent. Some people may experience only mild symptoms that respond well to treatment while other people may have more arduous symptoms that can last years and are less responsive to treatment. In adult patients with DM, there is an underlying risk of cancer. Your doctor should perform testing to identify your potential risk of cancer.
Your healthcare provider can provide you with the best information and can help address any question regarding your medical problem.
Resources
Our Affiliate
Other Resources
The following organizations provide reliable health information:
- American Academy of Family Physicians (www.aafp.org)
- The Myositis Association (www.myositis.org)
- National Organization of Rare Diseases (www.rarediseases.org)
- Canadian Organization for Rare Diseases (www.rarediseases.ca)
Epidermolysis Bullosa
Overview: What is Epidermolysis Bullosa?
The information in this section has been gathered from existing peer-reviewed and other literature and has been reviewed by expert dermatologists on the CSPA Medical Advisory Board.
Epidermolysis Bullosa (EB) involves a clinically and genetically diverse class of rare, inherited skin diseases that can cause the skin to blister and erode very easily. It can occur in both children and adults at any age, but usually begins in infancy or childhood. The incidence rate of EB is approximately 20 per million live births each year. EB affects both sexes equally and it is more common amongst the Korean/Asian populations along with African-Americans.
The human skin has many layers, which are held together with a wide variety of proteins that act like an adhesive glue. In EB, these proteins are either missing or short in supply. This allows for skin breakdown and damage when friction is applied against the surface of the skin. EB is caused by the genetic mutation of at least 20 genes which are necessary to develop these important proteins needed to maintain the structural integrity of the skin.
There are four types of EB, classified on a combination of the depth of the blister formation. These four categories are:
- Epidermolysis bullosa simplex: This is the most common variant of EB. It is the mildest form of EB, usually limited to the hands and feet. When friction is applied to the skin, the skin will split open causing blisters to form on the very top layer of the skin (epidermis).
- Junctional epidermolysis bullosa: The level of the skin that the blister can affect in junctional EB is the middle layer of the skin. This is a deeper level wound than in EB simplex.
- Dystrophic epidermolysis bullosa: In dystrophic EB, the skin is most fragile in the deepest layer or dermis. It is called “dystrophic” as it refers to the scarring of the skin that is noticed once the blister and erosions heal.
- Kindler Syndrome: This form of EB presents at birth or in early infancy. In addition to skin blistering, the skin of these patients is very sensitive to the sun.
Symptoms
For individuals born with EB, it can be first recognized at birth or during the first several weeks of life. The most prominent characteristic of EB is that the skin is fragile, which can lead to the development of blisters and wounds in the skin after mild trauma (e.g., injury from a bump or light friction).
The amount of blistering can vary from very little to quite extensive. The blisters are often localized to trauma-prone surfaces of the skin such as the elbows, knees, back of the hands, nails, feet, and toes as well as the diaper area in infants. The mucous membranes may also be involved. Blisters may form in the mouth, larynx and esophagus. There have also been reports of involvement of the eye, which in some reports has caused blindness. These blisters can be very painful and as mentioned previously, can result in scarring.
Treatment
Diagnosis
If your physician suspects a diagnosis of EB, he or she will perform a skin biopsy. The biopsy of a fresh blister will be sent to a laboratory so that the cells of the skin can be analyzed under a microscope by a trained healthcare provider (dermatopathologist). Once viewed under a microscope, a diagnosis of EB can be made based on the structural and histochemical features of the skin. It is important that fresh blisters be biopsied to accurately diagnose EB. Blisters more than 12 hours old should not be biopsied.
The healthcare provider may want to perform genetic testing to confirm more specifically the type of EB that you have. This is not a first-line diagnostic test for EB, because there is limited availability and high cost involved. Blood samples are obtained from the patient and his or her parents and sent out for genetic mutation identification at specialized facilities. Genetic testing is commonly performed in patients with Kindler syndrome, in newborns that are the first affected members in the family, and in families with a severely affected child.
Treatment
Depending on the type of EB, and the various parts of the body that are affected with blisters, different healthcare professionals can be involved in the care of the patient. This condition benefits from multidisciplinary care. The healthcare professionals that can be involved include: dermatologists, specialized EB nurses, pediatricians, geneticists, dentists, gastroenterologists, podiatrists, occupational therapists, dieticians, social workers and plastic surgeons.
There is currently no cure for EB. However, there are several important aspects of managing patients with EB:
- Preventing blisters: One of the primary goals in treating EB is to prevent blistering as much as possible. Blistering will be inevitable, but you want to limit the amount of trauma inflicted on the skin. It is important that individuals be dressed in soft clothing to avoid rubbing the skin against rough clothing material and seams. The tags of the clothing should be removed. Use padding on the surfaces the individual rests on as they can cause friction (e.g. chairs, beds, car seats).
- Wound care: Blisters should be popped with a sterile needle, as this can help facilitate the healing process and allow for greater patient comfort. After it has been punctured, keep the roof of the blister on the skin to improve healing. Place an appropriate solution, cream and/or dressing onto the blister after it has been drained.
- Infection control: Topical treatments and regular baths with or without bleach can help decrease the likelihood of a skin infection. If an infection is present, topical or oral antibiotics can be used for treatment.
- Diet: There are no dietary guidelines established for patients with EB. However, it is better if the food provided to the individual be soft so that there is a decreased chance of developing blisters within the lining of the mouth, throat and esophagus. EB patients with wounds present in their gut may require dietary supplementation of iron and other vitamins and minerals. Consulting with a dietician can help provide more thorough information.
Coping and Support
Coping
Patients suffering from EB experience a significant impairment in their quality of life. Patients have great restrictions in physical, social and sporting activities. They can also have limited employment and education opportunities if the condition is severe. Children with EB may have a more difficult time developing friendships and experience social isolation or psychological problems as their ability to participate in the physical aspects of a normal childhood experience is prevented by the pain they experience. Counselling may be needed to help cope with this disease.
Support
There is a tremendous burden on families with children that have EB. The primary support groups that exist to support families and patients living with EB are:
- Debra Canada (www.debra.org)
- Debra International (www.debra-international.org)
- EB Research Partnership (www.ebresearch.org/)
- EB Clinic at Sick Kids Hospital (www.sickkids.ca/areas-of-care/clinics/eb-clinic.html)
- EB Clinics at Sainte Justine Hospital (Pediatric) and at the CHUM (Adult clinic)
Resources
If you are living with Epidermolysis Bullosa, or know someone who is, you may want to stay up-to-date on the condition as well as current treatments and news.
Our Affiliate
 Debra Canada
Debra Canada Other Resources:
This section of our website is dedicated to the memory of Jonathan Pitre, a courageous EB patient and passionate advocate for EB and Debra Canada.

Fungal Infections
Overview: What are fungal infections?
The information in this section has been gathered from existing peer-reviewed and other literature and has been reviewed by expert dermatologists on the CSPA Medical Advisory Board.
Fungal infections are infections caused by fungi, organisms related to moulds, mushrooms and mildew. They live in the air, water and soil, and on plants. About half of all fungi are harmful to humans. Fungal infections are rarely life-threatening, but they can be contagious and can lead to a number of skin conditions, including:
- Athlete's foot
- Jock itch
- Ringworm
- Nail infections
- Scalp infections
- Candidiasis (thrush)
- Oral intertrigo
- Vulvovaginitis
- Diaper rash
- Paronchia
- Chronic mucocutaneous candidiasis
Each fungus has adapted in a particular way to thrive in specific parts of the body. For example, the fungus associated with nail infections lives on the keratin (protein) in the nail, whereas the fungus that causes athlete's foot lives on the dead skin between the toes.
 fungus-1
fungus-1  fungus-2
fungus-2  fungus-3
fungus-3
Risk factors for fungal infections include:
- Poor blood circulation (e.g., in persons with diabetes)
- High skin moisture content due to sweating, insufficient towelling off after a bath or shower, wearing tightly fitting or airtight clothing, walking barefoot in wet environments such as gyms, shower rooms or around swimming pools
- Excessive or deficient physical hygiene
- Damaged skin from wearing tightly fitting shoes
Symptoms
Because fungal infections can occur almost anywhere on or inside the body, their symptoms vary.
External Fungal Infections
Fungal infections that occur on the skin typically grow from the inside out, leaving skin broken and irritated or appearing as an inflamed round patch, as in the case of ringworm. Fungi can infect all body parts, such as the torso, arms, legs, face, hair, groin, soles of the feet, palms of the hands, and between fingers and toes. Some of the more common external fungal infections include nail infections, athlete’s foot and dandruff.
The symptoms of nail infections include:
- The tip of the nail turning yellow or brownish
- The spread of a yellow or brown colour over the nail
- The nail becoming very thick and brittle over time
The symptoms of athlete’s foot are:
- Cracking and peeling of skin between the toes
- Inflammation
- Areas of white, dead skin
- Moistness or blistering
- Itching or soreness
The main symptoms of dandruff are:
- Flakes of dead skin that appear in the hair and on the shoulders
- Itchy scalp
Internal Fungal Infections
Fungal infections can also occur inside the body, such as in the mouth, esophagus and vagina.
Infections in the mouth and esophagus are called thrush and are caused by Candida yeast. Candida can exist in the mouth and intestines without creating a problem, but it sometimes grows out of control, leading to the development of a white coating in the mouth and a clear mucous membrane with sores under it.
Vulvovaginitis, a yeast infection of the vagina, is sometimes hard to diagnose because its main symptom is a discharge, which is a normal occurence for most women. However, a vaginal yeast fungal infection has some specific characteristics:
- Pain during urination or sex
- A thick, crumbly, white, odourless discharge
Treatment
Due to the wide variety of fungal infections, your doctor will use different strategies to diagnose your condition. She or he may be able to diagnose it through observation or may wish to take tissue or blood samples if an internal infection is suspected. For this reason, it is best to make an appointment to see your doctor if you suspect you have a fungal infection.
Fortunately, a number of treatment options are available, ranging from proper skin care and lifestyle changes to medication.
Skin Care Strategies and Lifestyle Changes
You can take several steps to prevent fungal infections from starting in the first place or from recurring:
|
AVOID |
INSTEAD |
|
|
If you develop a fungal infection, there are several ways to manage your condition at home:
- Keep the affected area dry and clean by washing daily and drying between your toes and skin folds and (if on the scalp) blow-drying your hair.
- Clean the shower or bath using bleach.
- Wash socks, towels and bathmats at a temperature of at least 60 degrees Celsius.
- Regularly wash floors where you walk barefoot.
Medication
Treatment for the various fungal infections varies significantly depending on the type of infection (internal or external) and its location on the body. However, all treatments for fungal infections go right to the cause of the problem: the fungus. Antifungal treatments, whether applied to the skin or taken as a pill, kill or slow the growth of invading fungal cells to eliminate the problems they cause.
Topical Treatments
Antifungal drugs (e.g., terbinafine, clotrimazole, tolnaftate, ketoconazole, clioquinol) either kill or slow the growth of fungus. Most of these over-the-counter topical creams, sprays or lotions are used for three common fungal infections: athlete’s foot, ringworm and jock itch. Some are also used in other fungal infections such as pityriasis and thrush. Be sure to check the medication’s packaging to be certain it is effective against your type of fungal infection. These creams are applied directly to the affected area, usually, twice a day for two weeks or more, depending on the drug and the condition you are trying to treat. They should not be used around your eyes. Side effects vary among the drugs but may include skin irritation, peeling and blistering.
Miconazole is an over-the-counter antifungal drug that can be used for several classes of fungi, including yeasts. It is available in different formulations, which can be used in combination. For example, women with yeast infections affecting not only the vagina but also the surrounding skin can use a topical cream externally and a vaginal suppository internally. The cream is applied to the affected area, once or twice a day. A vaginal suppository is administered for one day/night. Common side effects include vulvovaginal burning, itching, irritation, pelvic cramping, swelling, hives, rash, and headache.
Selenium sulfide is an over-the-counter topical lotion used to treat infections by a specific group of fungi (Malassezia). These fungi are yeasts that can infect the skin, causing tinea versicolor (pityriasis), on the scalp, causing dandruff and seborrheic dermatitis. Usage varies by product so it’s best to follow the recommended treatment. Some people experience skin irritation. These lotions should not be used on broken or inflamed skin.
Systemic Treatments
Itraconazole is a prescription antifungal drug used to treat a variety of fungal infections. The capsules are taken orally, and the dose and length of treatment depends on the type and location of the fungal infection. Itraconazole should not be taken for nail or skin infections if you have congestive heart failure or you are pregnant, planning to become pregnant, or are breast-feeding. A wide variety of drugs may interact with itraconazole, so talk to your doctor. The most common side effect is a skin rash.
Ketoconazole is a broad-spectrum antifungal prescription drug that can be used for a wide variety of fungal skin infections. The standard dose is 200 mg per day, but your doctor will ensure you receive the dosage that suits you best. Be sure to tell your doctor about other drugs you are taking, because some may be unsafe when combined with ketoconazole. Also, do not eat grapefruit or drink grapefruit juice while you are taking ketoconazole. Common side effects include gastrointestinal upset, including nausea or vomiting.
Terbinafine is an antifungal prescription drug used in treating fungal infections of the fingernails and toenails (onychomycosis). It can also be used for common athlete’s foot, ringworm and jock itch if these conditions don’t respond to topical treatment. It is not effective against tinea versicolor (pityriasis). The drug should be taken as prescribed by your doctor. Oral terbinafine can cause liver damage, and you should not use it if you are pregnant or nursing.
Other Treatments
Ciclopirox nail lacquer and Eninaconazole are prescription antifungal drugs that are available as nail lacquer, to be used in treating fungal infections of the fingernails and toenails (onychomycosis). They should only be applied to the affected nails and the skin immediately surrounding the nails. Apply it daily, for up to 48 weeks. To complete the treatment, your doctor should remove the unattached nail once monthly. You may experience a mild rash on the exposed skin. A common side effect is contact dermatitis.
Dequalinium is an over-the-counter lozenge for mouth infections, including fungal infections such as oral thrush. Dequalinium is also provided as an oral paint. To use, suck on the lozenges slowly every two hours as needed, or spread the oral paint liberally over the affected area in the mouth. Some people may experience a mild allergic reaction.
*All information on medical treatments on this site is provided as an overview only. For a complete and up-to-date list of side effects, warnings and precautions, read the product’s package insert and consult your doctor or a pharmacist.
**If you are considering an alternative or complementary therapy, discuss it with your doctor first, and always be sure to keep your doctor up to date about any vitamins, supplements, or other forms of alternative treatment you are taking. Like any medication, alternative therapies can interact with other medications/treatments and, in some cases, have side effects of their own. Remember that “natural” does not necessarily mean “safe.”
Coping and Support
Because fungal infections are typically acute (sudden and short-lived), not chronic (long-lasting), they rarely have a major impact on a person’s quality of life. Most fungal infections are itchy and can, therefore, cause some distress and discomfort, but since they usually appear in out-of-the-way places, such as between the toes and in the groin, they are rarely a source of embarrassment. If fungal infections are caught quickly and treated consistently, they are usually cured.
Herpes
Overview: What is herpes?
The information in this section has been gathered from existing peer-reviewed and other literature and has been reviewed by expert dermatologists on the CSPA Medical Advisory Board.
Herpes is a common viral infection that causes uncomfortable blisters on the skin and mucosa. In 50 per cent of cases it lies dormant indefinitely in the body’s nerve cells, where it can later reactivate and cause further blisters. There are two main types of herpes virus: herpes simplex and herpes zoster.
Herpes simplex is the cause of oral and genital herpes, and herpes zoster results in chickenpox and shingles.
The herpes simplex virus (HSV) can be further divided into two types: Type 1 (HSV-1) and Type 2 (HSV-2). HSV-1 is most often responsible for cases of oral herpes, and HSV-2 is most commonly responsible for cases of genital herpes. However, HSV-1 can infect the genital area.
Both HSV types are characterized by the same pattern of infection. The primary infection occurs when the virus first infects an individual. In about 10 per cent of cases, sores or blisters develop. In others, there may be mild or no visible symptoms. The itchy, painful blisters break and form sores that eventually heal. The virus, however, remains in the body.
After a latent period during which the virus remains inactive, patients generally experience several subsequent infections a year. Over time, the severity and frequency of these recurrent infections decrease. Recurrent infections may be triggered by various factors, including fever, stress, excess sun exposure, trauma, or a menstrual period. They may also recur for no obvious reason.
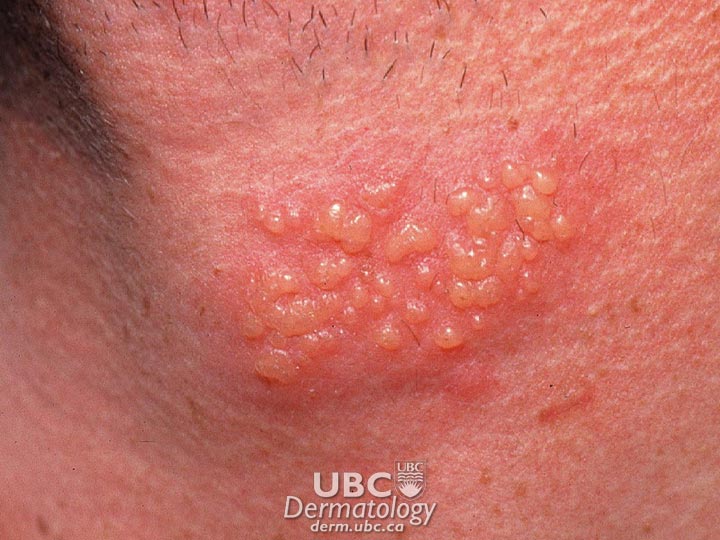 herpes simplex-1
herpes simplex-1  herpes simplex-2
herpes simplex-2
Herpes zoster is an acute, localized infection caused by the varicella-zoster virus, the same virus that causes chicken pox. After a chicken pox infection, the virus remains in some of the body’s nerve cells where it lies dormant (inactive) until reactivated. The reactivated virus travels along nerve fibres toward the skin, multiplies, and causes a painful, blistering rash known as shingles. Very rarely, shingles can lead to pneumonia, hearing problems, blindness, brain inflammation (encephalitis) or death. In some cases (usually in the elderly), a painful condition called post-herpetic neuralgia (chronic pain) persists after zoster disappears and can last for many months afterward.
Herpes is not dangerous in otherwise healthy individuals; however, the sores (if present) may be painful. In immunocompromised individuals and newborn babies, herpes can be serious but rarely fatal. Unfortunately, the virus may be spread even when there are no symptoms (asymptomatic shedding). Many infected individuals are not even aware they carry the virus.
 herpes zoster
herpes zoster  herpes zoster
herpes zoster
Symptoms
During the primary infection of oral herpes, these symptoms may occur:
- Small fluid blisters appearing on or inside the mouth or on the back of the throat
- Swelling of the lymph nodes in the neck
Symptoms may be mild or go unnoticed. Subtle symptoms may be mistaken for small cuts, bites or pimples.
In recurrent infections:
- When symptoms occur, they may appear as blisters or sores that generally heal more quickly than primary infection lesions.
- Many patients experience warning symptoms such as itching, tingling or pain 1-2 days before recurrences.
During the primary infection of genital herpes, these symptoms may occur:
- Some people develop one or two crops of sores or blisters within days, but sometimes within weeks or months of infection.
- Sores/blisters may appear on the penis or vulva, near the anus, or on the thigh and buttocks.
- Sores and blisters may break, ooze fluid, crust over, and heal in 2-4 weeks.
- Fever and swelling of the lymph nodes near the groin may occur.
- Headache and painful urination may be experienced.
- Some people develop minor or no symptoms.
These effects may appear in recurrent infections:
- Symptoms may appear as blisters or sores.
- Many patients experience warning symptoms such as itching, tingling or pain 1-2 days before recurrences.
{jkefel title=[Looking Deeper]}
In both HSV Type 1 and Type 2 cases, the infection follows the same course of action. During the primary infection, the virus makes multiple copies of itself, which mobilizes the body’s defences to fight the virus, thus limiting its spread. The defensive action may result in the characteristic sores and blisters or it may result in no visible symptoms. If present, the itchy, painful blisters break and form sores that eventually heal. The virus then retreats from the skin along nerve pathways to nerve cells where it establishes a small, permanent colony. During this resting phase (latency), the virus does not trigger the body’s defences. During the recurrent infection, the virus is reactivated, causing it to travel back down nerve pathways to the skin, where it triggers a recurrent infection. The virus again begins to multiply. This recurrent infection may result in sores and blisters similar to the ones exhibited during the primary infection; alternatively, there may be no symptoms.
{/jkefelend}
For both oral and genital herpes, transmission is by skin-to-skin contact when the virus is active. The virus is transmitted when a contagious area (lesion) comes into contact with breaks in the skin or mucous membrane tissue, usually in the mouth and genitals. The virus cannot breach intact skin.
- Most cases of oral herpes are transmitted during childhood by infected persons kissing or sharing eating utensils or towels with family and close friends.
- Most cases of genital herpes are transmitted during sexual contact with an infected person. It is possible for a person to contract genital herpes from oral sex with a partner with oral herpes.
- Both oral and genital herpes can be transmitted whether symptoms are present or not.
- Mothers can transmit genital herpes to their children during childbirth.
Herpes zoster is caused by reactivation of the varicella-zoster virus after a chickenpox infection. It is not clear what reactivates the virus, but a weakened immune system (which helps fight infection) may cause the virus to move along nerve fibres toward the skin where it multiplies and causes the symptoms to appear. Illness, trauma and stress may also be triggers that reactivate the virus.
If blisters break, the virus can be transmitted by direct skin contact to somebody who has never had chickenpox. That person will develop chickenpox, not shingles (although shingles can then occur later in life).
The herpes zoster virus typically results in the following symptoms:
- Reddish rash that turns into groups of blisters within a few days. Blisters crust and heal in 2-3 weeks. Most commonly, shingles occurs in a single area on one side of the body, in a strip or band of skin supplied by fibres from one nerve. This may show up as a banded rash wrapping one side of the trunk from spine to sternum.
- Burning, tingling pain, or skin sensitivity in one area on one side of the body. Pain may begin a few days before the rash and can range from mild to intense.
- Possible headache, fever, chills, nausea, diarrhea.
Complications following a diagnosis of herpes zoster include:
- Post-herpetic neuralgia (chronic pain). In about 1 in 5 cases, severe pain persists for months to years after the rash disappears. Elderly patients have a higher risk of developing post-herpetic neuralgia. Most people with post-herpetic neuralgia get better with time, usually within a year. A few people develop chronic, persistent pain.
- Herpes zoster ophthalmicus. Shingles of the eye causes swollen eyelids, eye redness and pain. Without prompt treatment, this can scar the eye, cause vision damage or lead to glaucoma, which can cause blindness.
- Ramsay Hunt Syndrome occurs when facial nerves are involved and includes facial paralysis, hearing loss, loss of taste in half the tongue, ear pain, and skin lesions near the ear and ear canal.
Treatment
A diagnosis of oral herpes is usually made following a visual examination by a doctor, though swab culture testing or blood tests may be performed to confirm the presence of HSV-1.
As the symptoms of genital herpes are variable, people with a lesion of any kind (blister, ulcer or sore) should see a medical professional for testing. A diagnosis of genital herpes is usually made following a visual examination, but swab testing may be conducted to confirm the diagnosis. Laboratory tests include microscopic examination and blood tests for antibodies to HSV-2.
Diagnosis of herpes zoster can be difficult before the blisters appear, but the sensation of pain in a band on one side of the body can be a clue. However, an accurate diagnosis typically follows the appearance of a rash combined with knowledge of a previous case of chickenpox or shingles. Testing is not usually needed but may include tests on blood or blister fluid.
There is no cure for either type of herpes infection at this time. However, a vaccine that may prevent herpes zoster has been approved. However, vaccines cannot treat shingles or post-herpetic neuralgia once they have started.
Although there is no cure for the virus, the symptoms of herpes can be treated.
Many patients with oral herpes choose not to treat cold sores unless the outbreaks are severe or frequent. Patients with genital herpes are more likely to undergo treatment. Three oral anti-viral medicines are approved for treatment of genital herpes:
- Acyclovir
- Famciclovir
- Valacyclovir
The drugs work by attacking the virus and disrupting its ability to multiply. All are safe to use; nausea and headache are the most common short-term side effects. No long-term side effects have been reported. Antiviral drugs are commonly prescribed for patients to treat primary infections, but they can also be used for recurrent infections. One of the drugs, valacyclovir, has been shown to reduce the risk of transmitting the virus to a partner.
Two kinds of treatment regimens are prescribed:
- Episodic therapy: Medication is taken at the first sign (even during the “warning symptoms” phase) of a recurrent outbreak and continued for several days. This speeds healing and may prevent an outbreak from being fully expressed. Some evidence indicates that there may be little benefit to taking the medication once lesions have appeared.
- Suppressive therapy: There are no approved oral anti-viral medications for oral herpes. For patients with frequent or severe outbreaks, some physicians will prescribe the oral anti-viral drugs approved for genital herpes. Two topical anti-viral medications (aciclovir ointment and penciclovir cream) are available by prescription to speed up healing of lesions and reduce viral shedding. Over-the-counter creams are also available, but only one, containing docosanol, has been approved and proven to speed healing.
Herpes zoster often disappears on its own. Treatment is usually directed at symptom relief with the following types of medications:
- Antiviral medications: If herpes zoster is diagnosed early, acyclovir or other antiviral medications may be prescribed to shorten the duration of the illness, minimize pain and reduce the chances of complications. Antiviral medications may also help those patients with compromised immunity or severe cases of shingles. Antivirals work best when started within 24–72 hours after the pain begins.
- Corticosteroids: Corticosteroids such as prednisone can reduce inflammation and lower the risk that post-herpetic neuralgia may develop, particularly in elderly patients. Corticosteroids are prescribed cautiously and seldom due to possible adverse effects.
- Analgesics (pain relievers): Mild pain may be controlled with over-the-counter medicines containing acetaminophen or ibuprofen. If pain is severe, a doctor may prescribe stronger medication.
- Antihistamines:Itching may be relieved by applying antihistamine creams or lotions topically (directly to the body) or taking antihistamine preparations orally (by mouth).
Natural treatments: A variety are available:
- Creams containing capsaicin (extracted from peppers) may help prevent post-herpetic neuralgia.
- Cold, wet compresses reduce pain.
- Oatmeal baths, starch baths and calamine lotion ease itching and discomfort.
In addition, researchers are exploring new methods for treatment for the herpes viruses and their complications. For example, the National Institute of Neurological Disorders and Stroke (NINDS) conducts shingles research. As well, new drugs and treatments may be tested now through clinical trials across Canada. To learn more about possible new treatments, visit our clinical trials page
Footnotes
*All information on medical treatments on this site is provided as an overview only. For a complete and up-to-date list of side effects, warnings and precautions, read the product’s package insert and consult your doctor or a pharmacist.
**If you are considering an alternative or complementary therapy, discuss it with your doctor first, and always be sure to keep your doctor up to date about any vitamins, supplements, or other forms of alternative treatment you are taking. Like any medication, alternative therapies can interact with other medications/treatments and, in some cases, have side effects of their own. Remember that “natural” does not necessarily mean “safe.”
Coping and Support
Helping Others Stay Safe
People with the herpes virus must take precautions to avoid spreading the virus to other people. During active outbreaks, people should keep affected areas away from other people until the symptoms have healed.
These steps are particularly important with genital herpes. Because genital herpes can be transmitted during and between outbreaks, patients should:
- Have their partner(s) undergo blood tests to determine if they have antibodies to the virus. Knowledge of a partner’s status helps couples to decide what steps are required to reduce the risk of transmission.
- Consider abstaining from sex or practise mutual monogamy with one uninfected partner.
Pregnant woman with genital herpes and who have active symptoms can transmit the virus to the baby as it passes through the birth canal. To prevent this, birth by Caesarian section is recommended. A doctor will advise the mother on the best form of delivery.
People with oral herpes must also take precautions:
- Never touch an open sore and then your eye, as it can result in herpes keratitis.
- Avoid touching a newborn baby, as newborns can be infected by exposure to HSV.
- Use condoms or other barriers during oral sex to reduce the risk of transmission.
People with herpes zoster will also need to be cautious. Shingles itself isn’t contagious, but the virus that causes it can be spread from a person with active shingles to a person who has never had chickenpox during the blister phase through direct contact with the rash. The person exposed would develop chickenpox, not shingles.
- The contagious phase is from blister onset to blister crusting.
- The virus is not spread through sneezing, coughing or casual contact.
- Somebody with post-herpetic neuralgia is not infectious.
The best thing to do is to lower the risk of contagion by covering the rash. Don’t touch or scratch the rash, and wash your hands often. Once the rash has developed crusts, you are no longer contagious.
During inactive periods, symptoms may not be present, but viruses may still be shed. With genital herpes, people should:
- Use latex condoms to protect the mucous membranes that are the most likely sites of transmission. Note that condoms do not cover all the potential sites for shedding (i.e., nearby genital skin).
- Consider undergoing daily suppressive therapy using valacyclovir, which has been shown to reduce the risk of herpes transmission.
- Develop good hygiene habits. The virus may be transmitted if the skin in uninfected areas is touched after contact with an open sore.
Psychological Care
The psychological stress of having herpes can vary depending on the type of virus a person has. For example, common reactions to a diagnosis of genital herpes (and its association as a sexually transmitted disease) include shame, depression or anger. These emotions often fade over time. In addition, some people may find it hard to adjust their sexual habits and lifestyle to prevent spreading genital herpes. For people experiencing emotional distress after a diagnosis, seeking professional support can help them to:
- Recognize that a genital herpes infection is a health issue, not a moral judgment.
- Develop a positive self-image and stop perceiving genital herpes as social stigma.
- Stop assuming that having herpes will prevent them from being romantically involved or having successful long-term relationships.
Professional counselling may also benefit people with herpes zoster if they are distressed over physical symptoms, lifestyle changes, or their personal appearance.
Physical Care
The physical impact of herpes on infected, otherwise healthy individuals is the pain and unsightly appearance of the blisters during outbreaks. The pain can be mild, as in the case of a minor oral herpes outbreak, to severe, as in the case of shingles.
People with herpes zostercan be intensely uncomfortable. Some people with shingles also develop post-herpetic neuralgia, a long-lasting pain that persists long after the rash has subsided. This pain can be severe enough to cause insomnia, weight loss, depression and preoccupation with finding pain relief. Both shingles and post-herpetic neuralgia can disrupt daily activities. Some people experience extreme sensitivity and find gentle touches, drafts and temperature changes unbearable. For these reasons, people with herpes zoster will want to work closely with a doctor to manage and alleviate their condition.
Regardless of the type of herpes virus a person has, pain and discomfort is best managed with the help of your doctor.
Hidradenitis Suppurativa
Overview: What is HS?
Hidradenitis Suppurativa (HS) is a skin condition that results in expanding tender lumps in the folds of the skin generally in the armpits and groin area. Painful skin lesions, nodules and boils can appear in these inflamed areas, and usually occur in areas of the body where certain sweat glands (known as apocrine sweat glands) are located. Other sites include areas under the breasts, on the buttocks and inner thighs, where the skin rubs together. Lumps that are close together can bond together under the skin.
It is estimated that over 1 million Canadians are currently living with HS, however, the exact number is not known since HS is often misdiagnosed and many who are living with HS don’t seek out a dermatologist for help.
Fast Facts
- Around 3.8% of Canadians have HS
- It is not contagious
- It can be hereditary
- It usually starts around puberty but it can start in childhood
- Stress management, loose clothing, losing excess weight and smoking cessation can relieve symptoms.
Causes
The exact cause of HS is not known. Multiple genetic and environmental factors appear to play a role. The onset around puberty suggests that hormones contribute to disease process probably through plugging of hair follicles where the apocrine sweat glands are located. HS is not an infection, rather it is a chronic skin condition. It is important to note that HS is not contagious and is not caused by poor hygiene.
HS commonly occurs in teens, young adults in their early 20s, but can occur at any age. Women are more likely to develop HS than men. Research has shown that HS may run in families, as 1/3 of HS patients have a family member who is also living with the condition. Other factors that can play a role in developing HS are smoking and being overweight.
HS can be associated with other conditions such as arthritis, severe acne, depression, metabolic syndrome, anemia and inflammatory bowel disease.
In 2017, The Canadian Skin Patient Alliance (CSPA) conducted a literature search and survey of patients with HS (formally diagnosed or self-diagnosed) to answer critical questions regarding gaps in patient care, and deficiencies in provincial healthcare systems. The focus of this research was to describe the patient experience from diagnosis and beyond, including a path to diagnosis, symptom control, experience with treatments, healthcare utilization, patient needs, and impact on the quality of life.
You can read this report here: Scarred for Life: A National Report of the Patient Experience Living with Hidradenitis Suppurativa
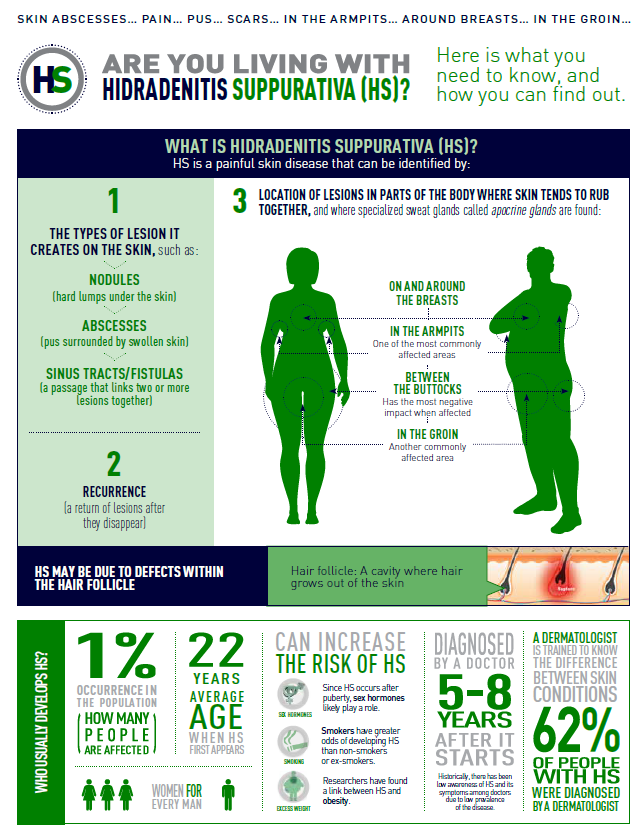
Symptoms
HS often occurs in armpits, groin, under the breasts, buttocks and on the inner thighs. HS can occur in one spot, or show up in multiple areas of the body.
Signs of HS can include:
- Blackheads - small pitted areas of skin containing blackheads
- Leaking wounds - these heal very slowly, if at all, and often lead to scarring and the development of tunnels
- Red Tender Bumps – these often grow in size and can break open, draining pus. This drainage often has an unpleasant odor. These bumps are found in areas where the skin rubs together. Itching and burning can also accompany these bumps.
- Painful lumps – these lumps are usually pea sized and hard. They develop under the skin, may persist for many years, enlarge and become inflamed
- Tunnels – over a period of time, tracts connecting the lumps can form under the skin. These wounds can heal very slowly, if at all, and can leak pus.
HS that is persistent and severe can lead to other complications including:
- Infection – the affected areas can have open wounds that become infected.
- Scars and changes in skin – the affected wounds may heal but leave scars, pitted skin or discoloured patches of skin that are darker than normal.
- Restricted movement – the sores, bumps, and scars can cause movement to be painful and limited. This is especially true when the disease affects the armpits or thighs.
- Obstructed lymph drainage – the most common sites where HS occurs are sites that also contain lymph nodes. Scar tissue can interfere with the lymph drainage system and can cause swelling in the arms, legs or genitals.
- Social isolation – due to the location, leaking sores and the odor produced by these sore, patients are often embarrassed and reluctant to go out in public. This can lead to sadness and depression.
- Cancer – very rarely, patients with advanced HS can develop squamous cell carcinoma in the affected areas.
HS can also be associated with other disorders such as metabolic syndrome (HTN, dyslipidemia, diabetes), arthritis, Inflammatory bowel disease, depression and anemia
Diagnosis and Treatment
Diagnosis
The diagnosis is clinical based on classic signs and symptoms and there is no test to diagnose the disease. Health care providers may in some cases run some tests to rule out an infection or other skin disorders. For severe cases, a dermatologist should be involved in the diagnosis and treatment.
Early detection of HS is important to getting effective treatment. Be sure to see your health care provider if your condition is:
- Painful
- Doesn’t improve in a few weeks
- Returns within weeks of treatment
- Appears in several locations
- Recurs frequently.
Treatment
There is currently no cure for hidradenitis suppurativa, but the goal of treatment is to achieve good control by reducing the frequency and severity of flare ups so the disease would have minimal impact on quality of life.
There are several treatment options available including medications and surgery that can help patients clear or reduce their breakoutsand prevent new breakouts. Talk to your health care provider about the risks and benefits of each to determine the best treatment option for you.
Self-care
Here are some simple measures to relieve discomfort:
- Apply warm compresses to help reduce the swelling
- Keep the affected areas clean
- Wear loose-fitting clothes to minimize irritation
- Weight optimization and smoking avoidance
- Keep a record of your triggers in order to avoid them.
Medications
Topical and oral drugs – These medications include antibiotics and drugs derived from Vitamin A (retinoids). These medications help reduce inflammation, fight infection and prevent HS from worsening. Antiandrogens can decrease the effect of sex hormones on the skin and they can be helpful especially in women with polycystic ovary syndrome. Corticosteroids can be injected into the lesions or taken by mouth to help reduce inflammation, however prolonged use of oral steroids may have additional side effects so their use is restricted to severe cases. Other oral medications that suppress the immune system can be helpful in some cases.
Pain Medication – if over-the-counter pain medications do not help relieve the discomfort of HS, your health care provider may prescribe something stronger such as codeine, morphine, fentanyl patch and others. Caution should always be used when taking prescription pain medication.
Biologics – Biologic medications known as TNF-inhibitors are showing promise in effectively treating HS. They are currently used to treat psoriasis, psoriatic arthritis, and other inflammatory conditions. They work by neutralizing an immune system protein known as tumor necrosis factor (TNF). They are usually administered by injection. Ongoing research is assessing these medications and there are several clinical trials under way for their effectiveness in treating HS. There is currently one biologic approved for the treatment of moderate to severe HS in Canada. Other biologics targeting alternative inflammatory molecules have shown some efficacy in small studies and they are sometimes used.
Coping and Support
HS patients often comment about how their condition impacts their day-to-day life including their personal relationships, their ability to work, physical pain, scarring and the self-care necessary to simply manage the disease. Others share the impact on their loved ones. Physicians are also learning more about the condition, which in time will lower the time-gap to a diagnosis. Many of those living with HS have learned to identify their triggers. With pain being one of the most common symptoms, patients are able to do their best to avoid a flare by avoiding known triggers.
HS impacts every aspect of patient life including the ability to maintain a career and personal relationships. A recent study indicated that two-thirds of patients with HS suffer from depression. Pain, depression, irritability all impact an HS patient's ability to develop healthy social supports with family and friends. On top of this, the disease has financial implications. Many patients spend hundreds, if not thousands, per year on bandages that are not covered under their health care plan.
The chronic nature of the disease makes it a difficult burden. You may feel embarrassed or anxious about your symptoms and become withdrawn, self-conscious or depressed. Family and friends can be a tremendous help as you go through challenging times, but you may find that you need additional support. A professional counsellor will be able to suggest various coping strategies. In addition, it can be useful to reach out to others who personally understand the challenges of HS. Hidradenitis & Me Support Group and HS Heroes are Canadian patient organizations, through them, you can connect with others who have lived a day in your shoes
Other Links:
Hsonline.ca
Hsfoundation.ca
Hs-foundation.org
Additional HS Resources:
Patient Summaries (Click to enlarge):
Impact on Personal Life Impact on Work-Life To Those Newly Diagnosed.


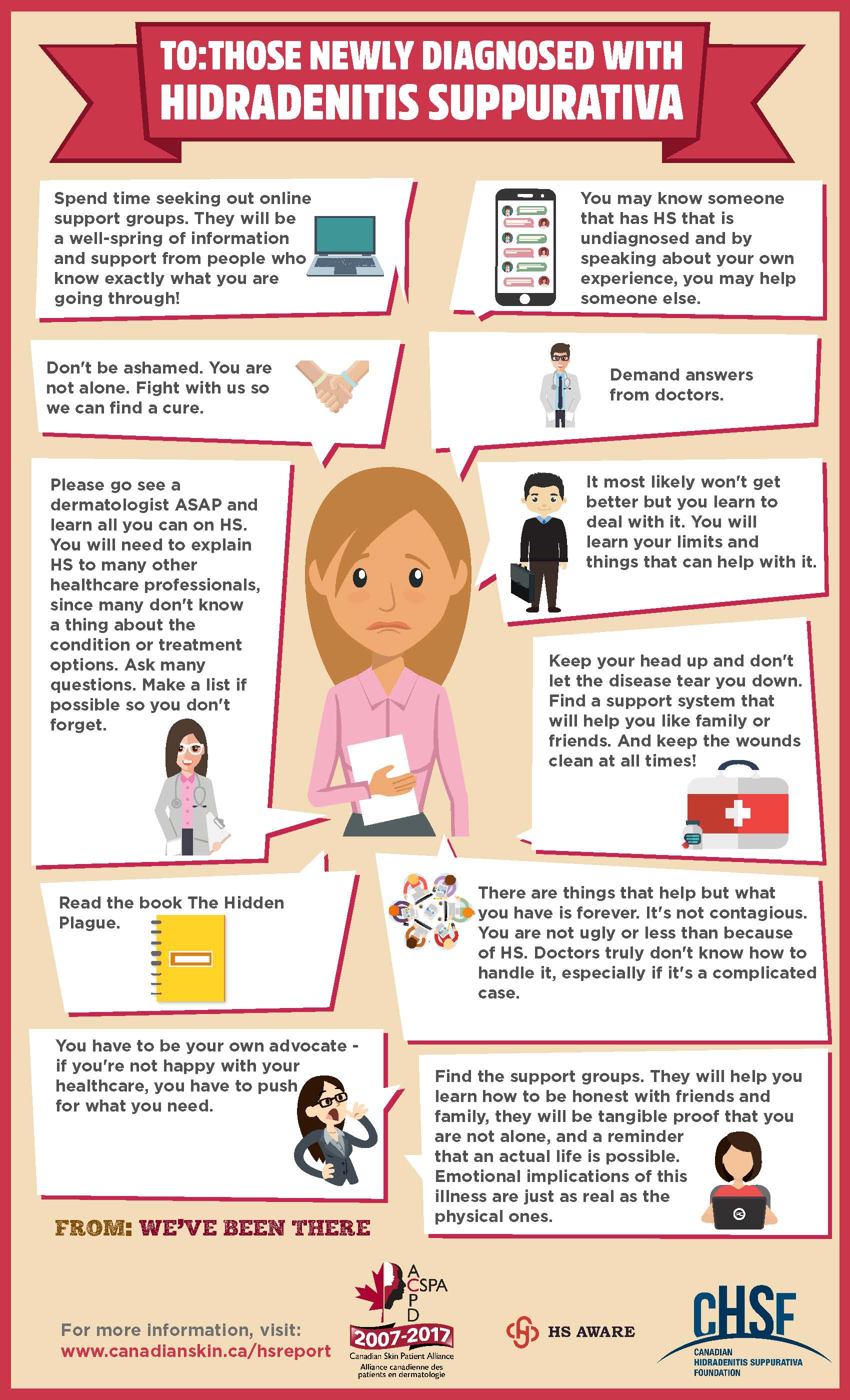
HS Infographics and Myth Busters (Click to Enlarge):
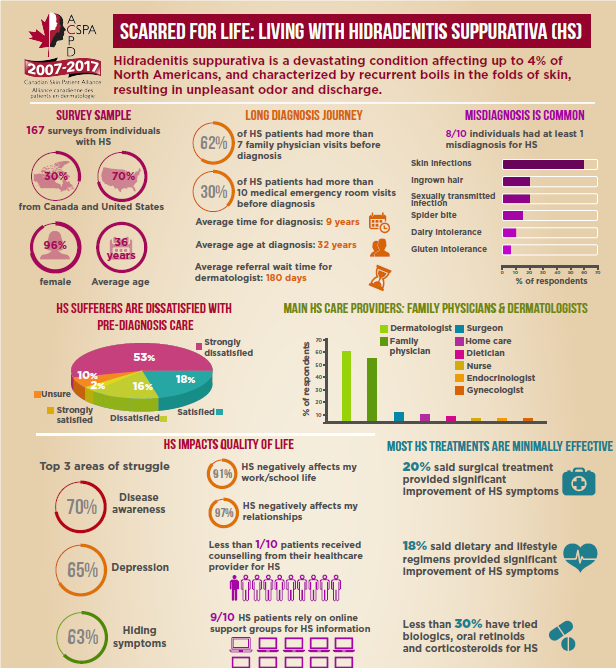
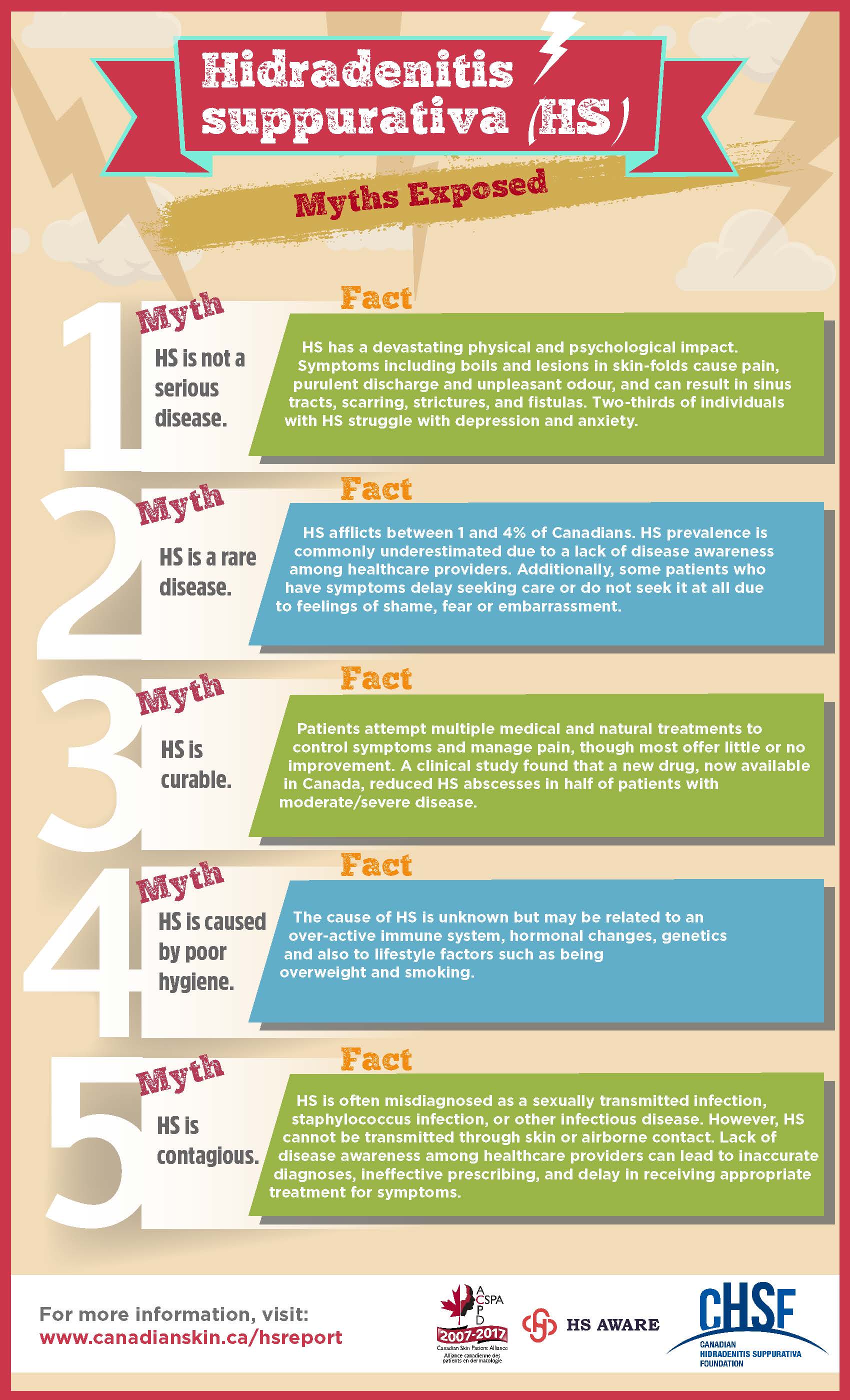
Radio spots:
680 News : May 6 2017 Interview # 1 680 News: May 6 2017 Inteview #2
Resources
If you are living with HS, or know someone who is, you may want to stay up-to-date on the condition as well as current treatments and news.
Our Affiliate Members:
![]()
![]()
Other Resources
The CSPA launched Scarred for Life: 2020 Update – A National Report of Patients’ Experiences Living with Hidradenitis Suppurativa in May 2020 to provide us with more information about the HS patient experience in Canada and abroad. We invite you to read the HS Report, view videos of patients, dermatologists, and mental health professionals, and learn more about the CSPA's work to improve health outcomes and quality of life for people living with HS in Canada.
HS Wound Care Video Series
HS Patient Decision Aid
This decision aid has six steps to guide you through the process of choosing which treatment option best suits you: https://www.informed-decisions.org/hidradenitispda.php
HS Awareness Week Webinar
Canadian HS Foundation - a foundation to help Canadian dermatologists better manage HS
Hidradenitis Suppurativa Decision Aid - a tool to help patients chose what treatment best suites them.
Infographics
Clinical Management Guidelines for HS

Impact on Personal Life Impact on Work-Life To Those Newly Diagnosed.
HS Infographics and Myth Busters (Click to Enlarge):
|
|
|||
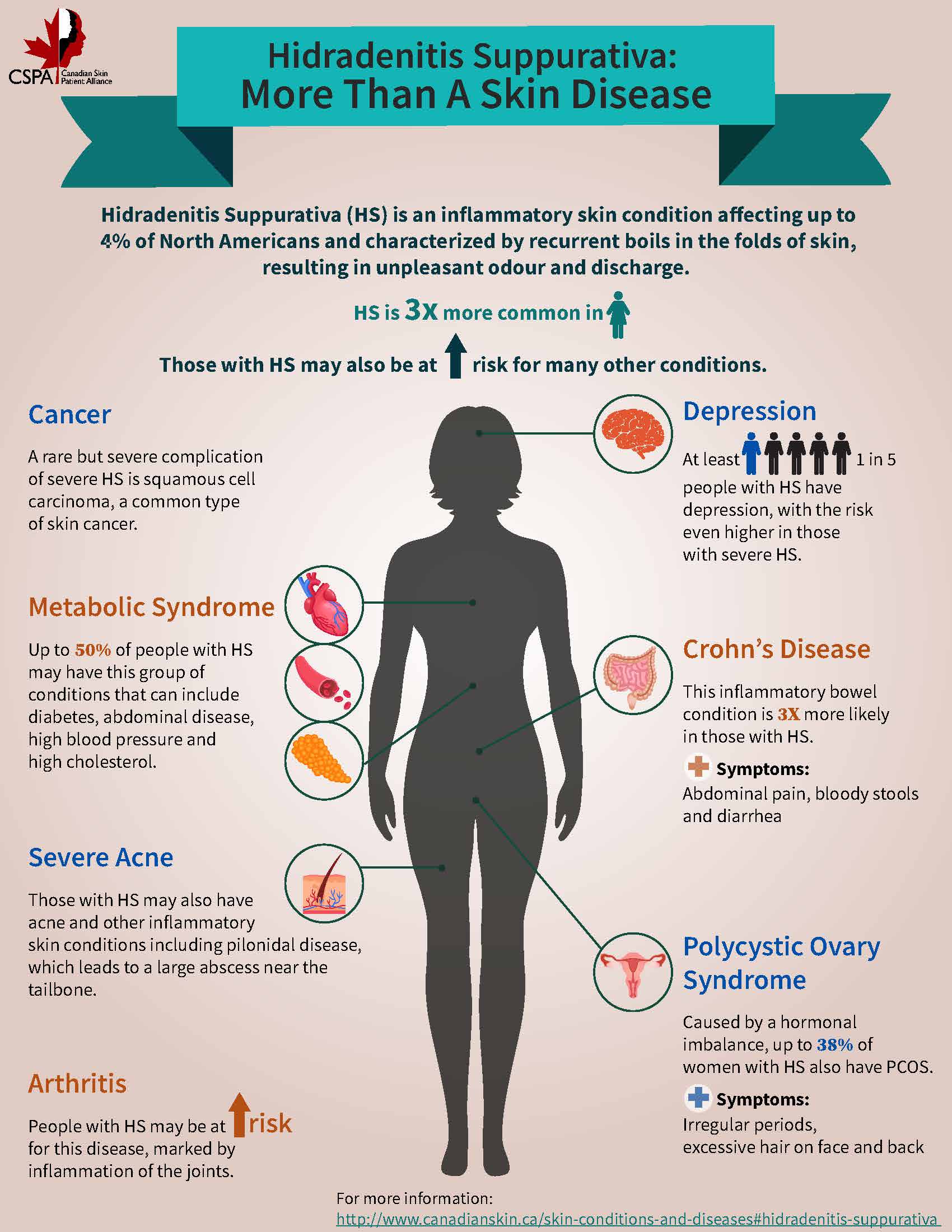
HS TED Talk - Bringing HS Out of the Dark - Jackson Gillies
Human Papillomavirus (HPV)
Overview: What is HPV?
The CPSA gratefully acknowledges Jessica Ho, MSc Public Health, MD candidate, Queen’s University, and Yuka Asai, MD, PhD for assistance in the preparation of this report. August 2021.
What is it?
Human papillomavirus (HPV) is a virus that is usually transmitted through skin-to-skin contact and sexual contact. It is a very common infection and an estimated 70% of sexually active women and men in Canada will contract sexually transmitted HPV infections in their lifetime (Government of Canada, 2020). It is most commonly contracted via sexual intercourse, including vaginal, anal and oral intercourse, and it is possible to contract HPV from a partner that does not have any symptoms.1 Other modes of transmission are possible, including transmission by touching a surface infected with HPV via fomites (objects or materials which are likely to carry infection, such as clothes, utensils, and furniture) and less commonly, children may develop HPV infections during birth via vaginal delivery or when in contact with a carer with an HPV infection.
There exists more than 200 different strains of HPV. Most HPV infections do not show any symptoms though some may present as warts and others can go on to cause different types of cancer. The majority of HPV infections resolve on their own without any intervention. The strains are generally divided into two categories; low-risk and high-risk strains. Some of the low-risk strains may be found on the skin such as warts on the body, hands, feet and around the genital area (also known as anogenital warts). High-risk strains have been associated with an increased risk for certain types of cancers including cervical, anogenital and oropharyngeal cancers (Table 1).
Table 1. Strains of HPV
|
Strains |
Effect |
|||
|
Low-risk HPV strains |
HPV type 1 |
Warts of the hands and feet |
||
|
HPV types 2 and 4 |
Common warts |
|||
|
HPV types 3 and 10 |
Flat warts |
|||
|
HPV types 6 and 11 |
Genital warts |
|||
|
High-risk HPV strains |
HPV types 16 and 18 |
Associated with precancerous lesions and development of certain types of cancer |
HPV infections from certain high-risk strains can be prevented with the HPV vaccine (see section Diagnosis and Treatment). Complications of high-risk HPV infections can include precancerous lesions, and potentially developing cancer itself. Cancer usually takes many years to develop after a person gets HPV.
Types of cancers that have been associated with HPV include:
- Anal
- Oropharyngeal (Throat)
- Cervical
- Vaginal
- Vulvar
- Penile
Very rarely, warts in non-genital areas can transform to a type of skin cancer known as squamous cell carcinoma. This is usually seen in populations that are already more susceptible to acquiring an HPV infection such as those with a compromised immune system.
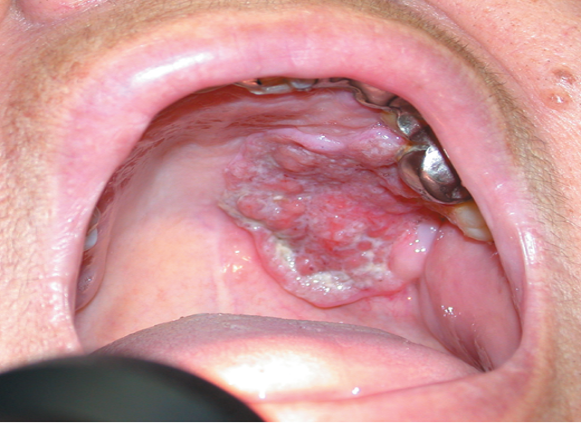
Image 1: Oropharyngeal cancer, associated with infection of a high-risk HPV strain.
Symptoms
While most HPV do not show any symptoms, some strains of HPV infection can lead to the development of warts on the body. Different types of HPV can lead to warts on different parts of the body, as well as in the genital region and in the mouth, usually from sexual contact.
Warts that are associated with HPV include:
- Common warts (verruca vulgaris)
- Filiform warts
- Flat plane warts (verruca plana)
- Plantar warts (verruca plantaris/ verruca palmaris)
- Periungual warts
- Butchers warts
More details about warts can be found here.
Non-genital warts
Warts may appear as fleshy skin-colored bumps (papules), scaly rough and hard (common warts), or thin and sticking out, with “church spire” peaks (filiform warts). Flat warts in particular may be difficult to see as they are skin coloured and quite flat to the skin; these can sometimes be itchy and lead to further spread of the virus from scratching. On the hands and feet, they may be thicker, and may sometimes be painful (palmoplantar/myrmecia). If these are grouped together, they can be called mosaic warts. Some areas can be more difficult to treat, like warts around the nails, known as periungual warts. Butcher’s warts are commonly seen in butchers or other people who handle meat.
 |
 |
 |
||
|
Image 2: HPV flat warts (verucca plana) around the mouth and lips area.(Photo courtesy of Dr. Irina Turchin)
|
|
Image 3: Plantar warts (verruca palmaris) on the palm of the hand. (Photo courtesy of Dr. Irina Turchin)
|
Image 4: Common wart (verruca vulgaris) on the back of the hand/finger. (Photo courtesy of Dr. Irina Turchin)
|
|
 |
 |
|||
| Image 5: Periungual warts around the nails of the toes. (Photo courtesy of Dr. Irina Turchin) |
Image 6: Plantar wart (verruca plantaris) seen as a verrucous plaque on the heel of the foot. (Photo courtesy of Dr. Irina Turchin) |
Genital warts
Genital warts are caused by certain strains of HPV and arise around the genitals and the anus, together they are sometimes known as anogenital warts. The size and number of warts may vary, and the color of the warts can range anywhere from a fleshy brown to a dull pink. Management of the warts depends on the size, appearance, location and number of warts present. More information on genital warts can also be found in our section on ‘Warts’.
Diagnosis and Treatment
Diagnosis
The diagnosis of HPV infection depends on the presentation of the patient and may often go undetected given many HPV infections do not have any symptoms. A diagnosis of warts from HPV infection is typically done by a physician and may be confirmed from a sample of the tissue by biopsy. Definitive diagnosis is based on the detection of the viral HPV DNA with laboratory testing, however, this is not done routinely in all patients.
Treatments
Treatment of HPV
Various treatments exist to treat HPV, and these have been summarized in Table 2.
Table 2. Summary of treatments available to treat HPV2
|
Patient-applied treatments |
Physician-prescribed treatments |
Physician-applied treatments |
||
|
● Salicylic acid
● Imiquimod
● Podophyllotoxin
|
● Retinoid cream (tretinoin)
● Cantharidin
● Immunotherapy medications
|
● Trichloroacetic acid (TCA)
● Podophyllin liquid
● Cryotherapy
|
Treatment of warts
Warts from HPV may disappear over time as the body mounts an immune response, and often resolve without treatment, particularly in children. Warts from HPV may be more resistant to resolving on their own in adults and in those with longstanding warts.
The choice of treatment often depends on the size, extent, and location of the wart, as well as patient preferences. Various treatments are available (Table 2), and two common treatments of warts include the use of topicals and/or cryotherapy.
Topical therapies such as salicylic acid are readily available over the counter and chemically exfoliate the skin cells to remove the wart. Thick warts are often soaked and pared-down prior to the use of a topical therapy to increase the efficacy of the treatment. Stronger concentrations of acid may be administered by a physician to treat warts.
Cryotherapy (cryosurgery) is administered by a physician and uses liquid nitrogen. Liquid nitrogen reaches very low temperatures and when applied, can effectively freeze the wart by penetrating into the basal layer of the skin to reach the virus. This may be repeated several times in one treatment. The size and thickness of the wart determines the number and length of treatments of cryotherapy. Potential adverse effects of this treatment include pain during the procedure, and it may result in lingering irritation, soreness, swelling, or the formation of a blister. Cryotherapy can sometimes be used in combination with topical over-the-counter treatments.
Consider involving the guidance of a healthcare professional before starting any treatments and always read instructions before using any medications. A full list of wart treatments can be found at our page on Warts.
Prevention of HPV infection
Human papillomavirus (HPV) vaccine prevents infection from certain strains of HPV that cause genital warts. An HPV infection can potentially lead to cancers of the cervix, the vagina and the vulva. The vaccine is given to girls and women, ages 9 to 26, and has recently been approved in men. Vaccination often requires three doses: an initial dose and boosters after two months and six months, however please refer to the Health Canada website to verify the recommendations for the vaccination schedule and dosing appropriate for your age group and population that you may identify with. The vaccine prevents HPV infection, but does not cure it. Because it is not 100% effective, and only covers certain high-risk strains of HPV, patients are still recommended to engage in safe sexual practices to reduce infection and transmission.
There are currently 3 approved HPV vaccines that cover strains that cause genital warts and that can lead to cancer. They are: Gardasil, Gardasil 9 and Cervarix.
Table 3. HPV vaccines available
|
Cervarix (HPV2) |
|
A bivalent vaccine which protects against HPV types 16 and 18 |
|
Gardasil (HPV4) |
A quadrivalent vaccine which protects against HPV types 6, 11, 16 and 18 |
|
|
Gardasil 9 (HPV9) |
A nonavalent vaccine which protects against HPV types 6, 11, 16, 18, 31, 33, 45, 52 and 58 |
Regardless of if they have been vaccinated, women should continue to have regular gynecological exams and Pap tests. Regular screening can detect cancers of the cervix, clitoris, or vulva as they often do not have any symptoms in the early stages. It is also recommended that individuals with anogenital warts be screened for other sexually transmitted infections (STIs). Partners should recommend that their sexual partners present to a healthcare practitioner if there are any symptoms present and that any partners with a cervix get regular checks and PAP smears.
Anal HPV may also occur and may present with symptoms and signs similar to genital warts. While it is less common than a cervical PAP test, anal PAP tests are available and involve putting a cotton swab in the anus to collect cells to examine for precancerous or cancerous changes. This is not routinely done as a screening for the general population in Canada but may be performed by a healthcare practitioner if you may be at an increased risk of anal HPV and cancer.
Treatment of cancer associated with HPV infection
If a patient develops cancer-related to an HPV infection, management may include modalities such as chemotherapy, radiation therapy, and surgery at the discretion of their healthcare team.
Coping and Support
Although HPV is a very common virus, the experiences that follow a diagnosis can be emotional for many patients. Aside from the discomfort and the treatments used to cosmetically improve the appearance (cosmesis) of warts, HPV infections may come with other adverse psychological impacts. Patients may be anxious about their diagnosis or worry about the potential consequences for their health as well as the potential to transmit the infection. While most HPV infections do resolve on their own without any specific treatment, seeking care for any symptoms is recommended to reduce the burden of disease. Practicing appropriate preventative measures can also reduce infection and transmission. Patients can reduce the risk of HPV infection by getting vaccinated against HPV, undergoing regular Pap screening, and engaging in safe sexual practices with their partner(s).
Seeking appropriate care for warts from a primary care physician or a dermatologist will limit the spread of HPV infections. Finally, treating HPV infections early may reduce the potential development of HPV-related conditions such as cancer. For patients experiencing psychological distress related to this condition, mental health resources and seeking appropriate care from a healthcare professional are good sources of support to cope with this common condition.
Resources
American Academy of Dermatology, Genital Warts, Diagnosis and Treatment - https://www.aad.org/public/diseases/a-z/genital-warts-treatment
American Sexual Health Association - http://www.ashasexualhealth.org/stdsstis/hpv/
American Cancer Society - https://www.cancer.org/cancer/cervical-cancer.html
American Society for Colposcopy and Cervical Pathology - http://www.asccp.org/Default.aspx
Centers for Disease Control and Prevention - https://www.cdc.gov/hpv/parents/questions-answers.html?CDC_AA_refVal=https%3A%2F%2Fwww.cdc.gov%2Fvaccines%2Fvpd-vac%2Fhpv%2Fvac-faqs.htm
Derm Net NZ - https://dermnetnz.org/topics/sexually-acquired-human-papillomavirus/
- Gravitt PE, Winer RL. Natural history of HPV infection across the lifespan: Role of viral latency. Viruses. 2017;9(10):1-10. doi:10.3390/v9100267
- Lopaschuk CC. New approach to managing genital warts. Can Fam Physician. 2013;59(7):731-736. http://www.ncbi.nlm.nih.gov/pubmed/23851535%0A http://www.pubmedcentral.nih.gov/articlerender.fcgi?artid=PMC3710035.
Ichthyosis
Overview: What is Ichtyosis?
The information in this section has been gathered from existing peer-reviewed and other literature and has been reviewed by expert dermatologists on the CSPA Medical Advisory Board.
Ichthyosis is an umbrella term referring to a grouping of over 20 different subtypes of rare genetic skin disorders characterized by dry skin that appears as dry, thickened and scaly. Ichthyosis comes from the Greek word for fish (ichthys), since it causes scaly skin similar to that of a fish. The epidermal (top) layer of the skin contains keratin proteins that accumulate to form a thick layer of hardened skin either because of decrease in the rate at which the skin sheds or because of abnormal production of proteins. This condition presents with a wide range of clinical changes from barely noticeable to very severe. Depending on the subtype there may be non-skin changes for which patients need to be monitored (see complications under the Symptoms tab).
Skin conditions included in the ichthyosis family include:
- Ichthyosis vulgaris
- X-linked ichthyosis
- Congenital ichthyosiform erythroderma, nonbullous (nbCIE)
- Epidermolytic hyperkeratosis (bullous ichthyosis, bCIE)
- Harlequin-type ichthyosis
- Ichthyosis bullosa of Siemens
- Ichthyosis hystrix, Curth-Macklin type
- Hystrix-like ichthyosis with deafness
- Lamellar ichthyosis, type 1
- Lamellar ichthyosis, type 2
- Lamellar ichthyosis, type 3
- Lamellar ichthyosis, type 4
- Lamellar ichthyosis, type 5
- Autosomal recessive congenital ichthyosis
- CHILD syndrome
- Conradi–Hünermann syndrome
- Ichthyosis follicularis with alopecia and photophobia syndrome
- Keratitis–ichthyosis–deafness syndrome
- Netherton syndrome
- Neutral lipid storage disease with ichthyosis
- Adult Refsum disease
- Ichthyosis and male hypogonadism
- Sjögren–Larsson syndrome
- Photosensitive trichothiodystrophy (IBIDS syndrome)
- Gaucher disease, type 2
- Ichthyosis acquisita
Symptoms
Symptoms usually worsen or are more pronounced in cold, dry environments and tend to improve or even resolve in warm, humid environments. Although symptoms range in severity and complexity from type to type, the main symptoms include:
- Dry, scaly skin
- Tile-like, small scales (see Image A)
- Scales colored white, dirty gray or brown — with darker-colored scales typically on darker skin (appearing on the trunk, stomach, buttocks, legs, face and scalp)
- Flaky scalp
- Deep, painful cracks in your skin
- Skin redness
- Blisters
- Peeling
- Itchiness
- Pain
- Tight skin

Complications due to the scaling of the skin include:
- Skin infections, especially with bacteria
- Dehydration
- Blocked sweat glands, which can lead to overheating
- Slow hair growth or loss of hair (alopecia) from scales on the scalp
- Burning more calories, because the skin has to work harder to turn over cells
Other complications include:
- Vision loss (due to corneal damage)
- Brain and nervous system issues
Diagnosis and Treatment
Diagnosis
An accurate diagnosis of ichthyosis can be made using a combination of methods. Depending on the type and severity, one or more of the following may be used:
1. Clinical examination by a dermatologist: Dry skin is a common finding in many skin related diseases. A dermatologist has the expertise to diagnose ichthyosis by looking at the extent of the dryness, type of scale and associated symptoms and signs (for example, redness) to determine if changes are related to ichthyosis or other skin disorders. Further work-up for a diagnosis may be required.
2. Genetic testing: Clinicians may try to establish the exact type of ichthyosis and patterns of inheritance using genetic testing. This involves collecting a small amount of blood and sending it to a laboratory for analysis. Genetic testing helps to identify the correct subtype of ichthyosis and counsel families on the risk of having other children with the same skin disease.
3. Laboratory analysis or a skin biopsy: Some types of ichthyosis may require a skin biopsy. To take a biopsy of your skin, a dermatologist takes a small patch of affected skin (lesion) and analyzes this under a microscope. Further laboratory techniques such as histopathology or electron microscopy can be used for more information about the condition.
Sources:
https://www.ncbi.nlm.nih.gov/pubmed/12553849
https://www.ncbi.nlm.nih.gov/gtr/conditions/C0079584/
https://emedicine.medscape.com/article/1198130-workup
https://www.mayoclinic.org/diseases-conditions/ichthyosis-vulgaris/diagnosis-treatment/drc-20373759
Treatment
Unfortunately, ichthyosis does not have a cure yet. Treatments do exist that can help relieve the symptoms and provide comfort to those affected. Applying creams, lotions and/or ointments daily (especially those containing lanolin, alpha hydroxy acids, urea, ceramides, cholesterol or propylene glycol) can help add moisture to the scaly areas. It is most advantageous to apply it soon after a shower or bath when the skin is still damp. Taking a bath in saltwater, rubbing the skin with pumice or removing dead skin with a product containing salicylic/glycolic/lactic acid may also help. The use of a portable humidifier to add moisture to the home could alleviate symptoms as well. Patients prone to overheating may benefit from avoiding heat and using cooling vests. If the symptoms are severe, medications such as acitretin or isotretinoin may be prescribed to help with dryness and scaling.
Coping and Support
The appearance of ichthyosis may cause those affected to become self-conscious. They may feel depressed, have low self-esteem, and/or not want to be seen. The pain and itching associated with ichthyosis may disrupt sleep or everyday activities, causing irritability and poor school/work performance. To help with any emotional problems, therapy groups or individual therapy sessions may be attended. The support of family and friends is helpful as well. Following proper self-care and routines to alleviate symptoms is crucial to optimizing quality of life when living with ichthyosis.
Reflections: Christine's Story
Christine Butler is a retired public servant who now serves as a municipal councillor in her hometown of Conception Bay South, N.L. She is the Co-Chair of the CSPA Board of Directors and additionally volunteers for organizations in her community concerning children, families and mental health/suicide awareness. Christine's favourite role is being "Nanny Christine."
Christine was born with a rare skin disease called recessive congenital ichthyosis erythroderma (CIE). When she was officially diagnosed at age 21 she started on the road of learning all things ichthyosis. “I don’t know that I can say I was happy to be born with this rare skin disease, but I do know … that having this disease has made me strong, has made me do things … has made me reach and go beyond goals I might not have otherwise. I have grown to be a confident woman who has had many achievements in family, work and the community."
Christine freely shares her story of living with ichthyosis through social media forums around the world in an effort to support other skin patients.
If you would like to share your personal patient story, please contact This email address is being protected from spambots. You need JavaScript enabled to view it..
Resources
Other Resources American Academy of Dermatology (USA) - https://www.aad.org/ American Society of Gene and Cell Therapy (USA)- https://www.asgct.org/ Coalition of Skin Diseases (USA) - http://www.skincoalition.org/ DermWeb (BC) - http://www.dermweb.com/index.htm National Organization for Rare Disorders (USA) - http://www.rarediseases.org/
Impetigo
Overview: What is Impetigo?
The information in this section has been gathered from existing peer-reviewed and other literature and has been reviewed by expert dermatologists on the CSPA Medical Advisory Board.
Impetigo (pronounced im-peh-ty-go) is a bacterial infection of the outer layers of skin, commonly caused mainly by Staphylococcus aureus and sometimes by Streptococcus pyogenes bacteria. It can spread through direct skin contact with the infected person, or by touching objects that have been previously used by the infected individual. Impetigo frequently appears in young children under 6 years of age and is contagious, with the infection often being itchy and painful. Adults too can get it, although the majority of cases are seen in children.
There are two types of impetigo:
- Nonbullous impetigo – This is the most common type, accounting for 70% of all impetigo cases. They can be caused by S. pyogenes or S. aureus bacteria. The condition is characterized by red, oozing sores that eventually develop a yellow crust. It usually affects the face, head and neck areas.
- Bullous impetigo - This type is less common, and is more often seen children. It is caused by toxins produced by S. aureus that will lead to blistering of the skin. This type of impetigo is distinguished by large, flaccid sores. For example in children wearing diapers, sores appear in the buttocks region.
Individuals impacted typically have skin that show prior signs of irritations. Some causes and risk factors are as follows:
- Scrapes and cuts
- Insect bites
- Scratching
- Eczema
- Poison ivy
Symptoms
Although symptoms can vary, generally, red bumps or sores appear that cause itchiness and ooze yellow fluid for both bullous and non-bullous impetigo. Sores can range in size - they can be as small as a pimple or as big as a coin.
Diagnosis and Treatment
Diagnosis
Doctors are able to confirm a diagnosis of impetigo by assessing the distinct red sores. There are usually no need to conduct laboratory tests. Sometimes, doctors may inspect the liquid from the sores to determine specific types of antimicrobial treatments that could be prescribed.
Treatment
Impetigo can heal by itself over the course of several weeks without any scarring left behind, but specific treatment options are usually necessary and will help relieve discomfort associated with the condition.
Two main treatments options are commonly prescribed:
- Topical antibiotics – They come in the form of creams or ointments and can be applied only to particular areas as deemed fit.
- Oral antibiotics – These are prescribed for large bullae such as those found in bullous impetigo, when the affected areas are extensive or when topical antibiotics are not helping.
Other options in conjunction with standard treatments:
Some studies have shown that non-antibiotics treatments like disinfectant soaps could help relieve some discomfort. Wet compresses some 20 minutes twice a day may help dry out the lesion faster. Hydrating creams or lotions can also help alleviate symptoms.
Prevention
- Wash hands - Good hygiene is the best way to avoid infection
- Keep nails clean and trimmed
- Minimalize skin contact with those infected, or refrain from touching objects used by the affected individual
- Avoid scratching any infected regions to prevent the infection from spreading
Coping and Support
The condition can prove to be embarrassing for both adults and children alike. Family physicians are the best point of contact for any questions or concerns. When deemed appropriate, referrals can be made by the primary care physician to a dermatologist.
Melasma
Overview: What is Melasma?
The information in this section has been gathered from existing peer-reviewed and other literature and has been reviewed by expert dermatologists on the CSPA Medical Advisory Board.
Melasma is a skin condition in which dark patches develop on both sides of the face. The distribution of patches is symmetrical and most commonly appears on the forehead, cheeks, nose, upper lip and chin. It will not spread to other areas of the body and it is not contagious.
The patches are caused by increased amounts of melanin (skin pigment) in the skin. The excess melanin may be located in the top layer of the skin (epidermis), in the middle layer (dermis), or both. The location of the pigment is an important factor when considering treatment options.
The condition may run in families and occurs mainly in women of child-bearing age. The condition has also been called the “mask of pregnancy,” as it tends to appear during pregnancy. After pregnancy, the mask often fades but may recur with subsequent pregnancies.
Melasma is also more common in people with darker skin types, especially Hispanics and Asians.
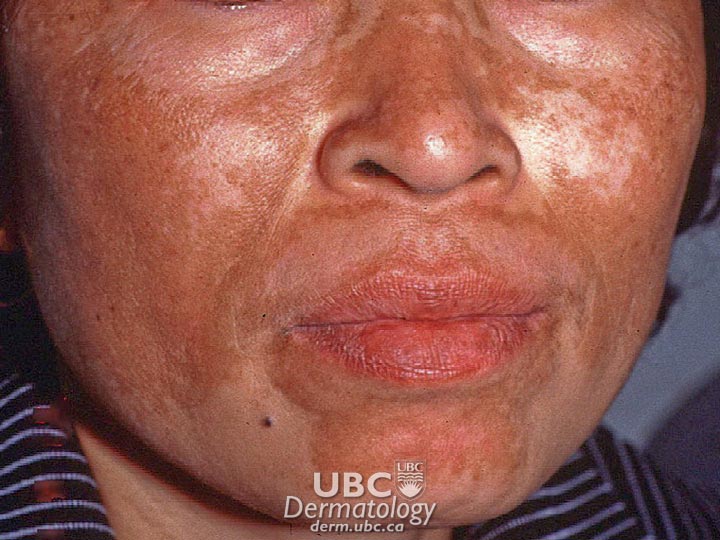 melasma-1
melasma-1  melasma-2
melasma-2
Causes
Though the mechanisms that trigger melasma are still under investigation, there appears to be a direct relationship with female hormonal activity, as the condition is common among women who are pregnant and those who use oral contraceptives. Certain medications or cosmetics may also cause skin darkening. Sometimes a thyroid gland dysfunction can contribute to the condition.
The most important cause appears to be sunlight exposure. The ultraviolet radiation in sunlight stimulates the overactive melanocytes to produce more melanin than the normal melanocytes in surrounding skin. Further exposure of the affected patches can cause additional darkening and, during treatment, can cause potentially successful treatments to fail. Some individuals may have a genetic susceptibility to developing melasma. More than 30 per cent of people with melasma have a family history of it, and there are reports of the condition affecting identical twins but not other siblings under similar living conditions.
In general, the condition tends to persist, though treatments are available to gradually lighten the darkened skin.
Symptoms
The symptoms of melasma include dark, irregularly shaped patches on sun-exposed areas of the face. Tan to brown patches indicate that the majority of pigment is in the epidermis (the outer-most layer of skin visible to the eye); blue or black patches indicate that the majority of pigment is in the dermis (the middle layer of our skin).
The distribution occurs in one of three patterns:
- centrofacial (across the centre of the face)
- malar (over the cheeks)
- mandibular (over the lower jaw)
Diagnosis and Treatment
Your doctor will diagnose the condition through a physical examination and a medical history. A thyroid test may be conducted to rule out thyroid disease. Examinations are often done using a Wood’s lamp or light, which shines ultraviolet light onto your skin. This will help your doctor identify whether the affected melanin is in the dermis or epidermis. (However, this type of light cannot be used accurately on people with dark brown skin.) Your doctor may also ask if you experienced any inflammation before the dark patches appeared, have been exposed to chemicals, or have been taking any medications that might cause pigment deposition.
Your doctor will also want to rule out other conditions that can cause the patches, such as menopausal changes, certain types of ovarian tumours and disorders such as Addison’s disease.
Melasma cannot be cured, and many cases require no treatment at all. For example, the melasma associated with pregnancy usually fades slowly after delivery; similarly, dark patches will fade eventually after discontinuation of oral contraceptive use. It will likely recur upon subsequent pregnancies or when restarting use of the contraceptive.
Cases of melasma where the melanin is in the deeper layer (dermis) are slower to resolve than cases in which melanin is restricted to the epidermis, as pigment deposited in the skin’s deeper layers cannot be physically removed. Treatment of dermal melasma aims to prevent the melanin in the dermal layer from being replenished. This results in very slow fading of the pigmented areas. In all cases, strict avoidance of sunlight is crucial to successfully resolving melasma and preventing resistant cases or recurrences.
Treatments for melasma include:
Topical Depigmenting Agents
- Hydroquinone (HQ) is a chemical that interferes with the process that melanocytes use for producing melanin. Formulations with higher amounts of HQ are more effective than those with lower amounts; however, adverse side effects increase with drug concentration. Side effects include skin irritation, sensitivity to light, and hyperpigmentation (darkening of the skin), some of which may be irreversible. Tretinoin (trans-retinoic-acid) is thought to increase the turnover of skin cells in the epidermis, which limits the transfer of melanin to the skin. Tretinoin is often used in combination with HQ as response is slow when tretinoin is used alone. Its side effects include skin irritation, temporary sensitivity to light and hyperpigmentation.
- Azelaic acid reduces melanocyte function. Unlike HQ, azelaic acid seems to target only hyperactive melanocytes. Normal melanocytes in light skin will not be affected. The primary adverse effect is skin irritation.
- Other depigmenting agents under study include 4-N-butylresorcinol, phenolic-thioether, 4-isopropylcatechol, kojic acid, and ascorbic acid.
Chemical and surgical peels
Chemical peels, microdermabrasion, and laser surgery have all been used to remove the layer of skin with the malfunctioning melanocytes. Results are obtained quickly but are unpredictable and may be temporary, as the melanocytes on the new skin may also malfunction. Such procedures can also irritate the skin, which can worsen melasma. Some physicians combine mild exfoliation with topical depigmenting agents. A number of studies have found this to be safe and effective.
Coping and Support
Melasma does not impact a person’s overall physical health. However, people with the condition may feel embarrassed, depressed or anxious due to their skin’s appearance. These feelings may lead to social isolation and loneliness and can be addressed by speaking with a psychologist.
To manage the physical symptoms of melasma, some people choose to cover the darkened patches with cosmetics. To prevent further damage, people with the condition must use sunscreen, even on cloudy or hazy days. A sunscreen that has a rating of 30 SPF or higher and that protects against both UVA and UVB rays is recommended. Some people with melasma use tanning beds in an effort to “even out” the appearance of their skin; however, this does not work, and tanning beds must be avoided as they can make the condition worse and have other dangerous side effects.
Nail Fungus
Overview: What is Nail Fungus?
The CPSA gratefully acknowledges Yuliya Lytvyn, PhD, MD candidate, University of Toronto, Richie Jeremian, PhD, MD Candidate, McGill University, and Charles W. Lynde, MD, FRCPC, DABD, FCDA for assistance in the preparation of this report. June 2021.
Nail fungus affects about 8% of Canadians. In 90% of patients, it is caused by fungi (dermatophytes) and less commonly by yeast (Candida). The fungus usually invades the nail at the free edge and then spreads down the side toward the base. Less often, it starts from the base and moves upward. Infection may also occur in patches or streaks on the nail surface. Nail fungus infections are progressive, recurrent, and contagious. Therefore, nail fungus is challenging to manage due to difficulty in diagnosis, frequent recurrences, long-term treatment periods, and potential side effects of oral medications.
Symptoms
The signs of a nail fungus infection are:
- Separation of the nail from the nail bed (onycholysis)
- Debris (dirt, dead skin cells, etc.) under the nail
- Discolouration of the nail (usually white or yellow, sometimes brown)
- Crumbling or destruction of all or part of the nail
- Odour coming from the nail bed
- Thickened and crumbling nails, often with ridges
- Numbness, tingling or pain in or below the nail
- May involve a single nail, but more frequently multiple nails
- Fungal infections affect toenails more often than fingernails, as fungi grow better in a warm and moist environment (often covered by socks and shoes).
Nail fungus is not simply a cosmetic problem; it is an infection that is contagious and can cause pain, discomfort and issues walking and moving, and could potentially lead to serious complications. Nail fungus infections are most often caused by fungi found in soil and decaying plants. This family of organisms can also cause fungal infections of the skin, and it is possible for a fungal infection to spread from the skin to the nails, or vice versa.
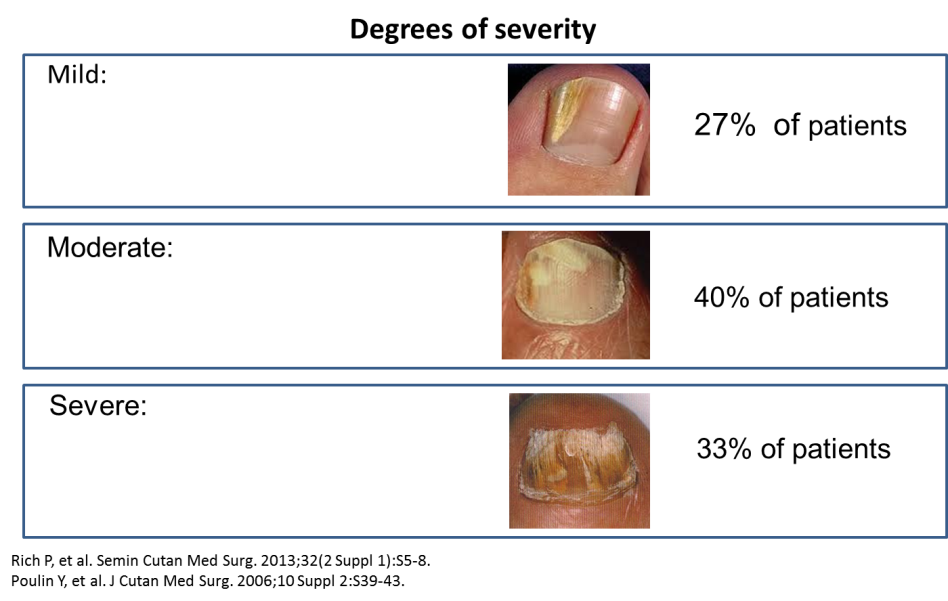
Diagnosis and Treatment
Diagnosis
Your physician will examine your nails and may send a small clipped sample for testing. Tell your physician how long you have had this condition, what treatments you may have tried so far, and how nail fungus has affected your day-to-day life.
Several factors unique to modern life have resulted in an increased prevalence of nail fungus. Patients can come into contact with the infecting yeasts or molds in many ways:
- Going barefoot in public areas, such as swimming pools and gym locker rooms or showers
- Getting your nails done in a nail salon where proper hygienic practices are not observed.
- Wearing shoes that trap moisture and warmth, particularly fashionably tight, high-heeled shoes
Other risk factors for nail fungus infections include: previous nail injury or trauma, skin infections, contact with infected household members, psoriasis, family history, poor circulation, smoking, and genetic predisposition. Moreover, the number of affected patients is much higher in those over age 55 and individuals with certain medical conditions such as HIV/AIDS, diabetes and psoriasis. Men have a 2.4 times greater risk of developing a nail fungus infection than women. Other contributing factors include a history of athlete’s foot and excessive sweating.
Treatment
Fungal infections can be difficult to cure, and treatment depends on the severity of the symptoms, the specific infectious organism, extent of nail involvement, side-effects of treatment, associated costs, and patient preference. Patience is required with treatment as it may take as much as 12 to 18 months for a healthy nail to grow out and for nail appearance to improve. A “true” fungal infection can only be diagnosed by a physician after obtaining appropriate nail cultures. Consult your doctor if you suspect you have nail fungus.
- Over-the-counter treatments:It is unlikely that an over-the-counter remedy will properly treat nail fungus. More importantly, the use of such remedies may delay appropriate treatment.
- Prescription topical treatments:Topical therapy is the first-line treatment for patients with mild-to-moderate nail fungal infections. These topical agents are applied directly to the nail and are relatively safe, with the most common side effect being irritation from certain ingredients in the treatment, such as alcohol. Topical nail fungus treatment options include ciclopirox and efinaconazole. Rarely, a low-dose topical corticosteroid may be prescribed for an anti-inflammatory effect, although it is avoided in most cases. The disadvantage of topical therapy could be a longer treatment time period and decreased effectiveness in extensive disease with more severe nail involvement.
- Prescription oral therapy is preferred for treating severe nail fungus infections, but they may not be suitable for some patients because of drug interactions (especially in older adults) and other safety concerns (e.g. liver toxicity). Additionally, some medications are contraindicated in women who are pregnant or patients with heart disease. Other side effects may include headaches, taste disturbances, and an upset stomach. Always notify your doctor of all your health conditions to reduce the risk of side effects or contraindicated use of medication. Options for oral antifungal therapy include terbinafine, itraconazole, or fluconazole. Advantages of oral therapy include shorter treatment time periods and greater effectiveness compared to topical therapy.
- Nail removal:With or without other treatments, your physician may suggest having your nail removed. Chronic pain may require permanent removal of the nail.
- Laser treatment:A fairly new treatment option is light therapy, commonly performed at a medical clinic. It is a relatively expensive treatment option with limited evidence. Studies are still being done to confirm the exact effectiveness of this therapy. Speak with your doctor to discuss if this option is suitable for you.
- Photodynamic therapy: Very limited data exists regarding successful use of photodynamic therapy to treat nail fungus. As more data becomes available, this may become a viable treatment option.
- Surgery: Surgical removal of the nail is performed for patients who do not respond to any other treatments. After surgery, topical or oral treatment is usually started to prevent recurrence.
- Symptoms relief with topical urea: Thick, deformed nails may make it difficult for patients to trim nails and could cause pain. Topical urea may be applied either alone or in addition to treatment above to decrease nail thickening.
Unfortunately, all treatments have relatively high failure rates due to inaccurate diagnosis, resistance to drugs or patients not adhering to therapy. For most optimal results, it is critical for patients to take medication as prescribed for the full-time course.
Coping and Support
Despite availability of topical and oral therapy, recurrence of nail fungus infection is very common (in approximately 20-50% of all patients), especially on toenails and when the degree of nail fungus is severe. In patients that have recurring fungal nail infections, occasional topical and oral antifungal therapy may be initiated.
If left untreated, infection may spread to other nails. Nail fungus infections can lead to serious complications, like skin infections (i.e., cellulitis), especially in patients with diabetes or other conditions or treatments that compromise the immune system.
Tips to help prevent nail fungus
- Keep your feet clean and dry.
- Avoid nail polish and acrylic nails, which prevent air from reaching the nail surface.
- Avoid sharing unsterilized nail manicure equipment.
- Avoid walking barefoot in public showers, pools and locker room areas – instead wear sandals or flip flips when in these areas.
- Change shoes and socks frequently.
- Keep nails clipped short and straight across.
- Wear well-fitting socks and shoes made of breathable materials (cotton, wool, new moisture-wicking fabrics).
- Old shoes may often harbor large numbers of infectious organisms and should be discarded or treated with disinfectants or antifungal powders.
- Disinfect clippers and other instruments used to treat nails.
- If prone to fungal infections, consider using antifungal or absorbent powders.
- Inspect your hands and toenails regularly to identify and treat nail fungus early.
If you suspect you have nail fungus, do not hesitate to speak to a healthcare professional. The pain and discomfort related to nail fungus is best managed with the help of your doctor.
Are you hiding your hands or feet due to embarrassment? Nail fungus is common and treatable. Do not let it burden your life.

Nails - Other Disorders
Overview: What are nail disorders?
The information in this section has been gathered from existing peer-reviewed and other literature and has been reviewed by expert dermatologists on the CSPA Medical Advisory Board.
Nail disorders refer to changes in the appearance or condition of healthy nails, which are smooth and hard with an even colour. Irregularities such as white spots or vertical ridges on a nail’s surface are harmless.
In some cases, nail disorders are considered minor yet may require treatment as they can affect everyday tasks such as walking, holding objects, and fastening buttons. However, it is important to note that changes to nails may also signal significant damage to the nail and surrounding tissue, or a more serious underlying disease that requires a visit to the doctor. For example, a red nail bed can indicate the presence of an underlying heart condition, and thick yellow nails can signify lung disease. Generally, you should visit your doctor if you notice any of the following in your nails: changes in colour or shape, swollen skin or pain, white or black lines, or dents or ridges.
The information below focuses on three of the most common nail disorders: onychomycosis, paromychia and ingrown nails.
Onychomycosis is caused by fungi, most commonly dermatophytes and less commonly, yeast (Candida). The fungus usually invades the nail at the free edge and then spreads down the side toward the base. Less commonly, it starts from the base and moves upward. Infection may occur in patches or streaks on the nail surface.
Paronychia results when injury to the nail causes the nail to separate from the nail fold and allow the entry of bacteria, most commonly Staphylococcus aureus or Streptococcus species. A mixture of bacteria may be present, particularly in persons with diabetes. Greenish nails suggest Pseudomonas species infection. Chronic paronychia is caused mainly by yeast fungus (Candida).
Ingrown nails occur when the corners or sides of a nail curve and dig into the flesh and an inflammatory response ensues. Ingrown nails may be caused by:
- Improperly trimmed nails (nails should be trimmed square and straight across, to the tip of the toe only using toenail clippers).
- Heredity, which may determine the curvature of nails.
- Tight shoes that crowd the toes.
- Repeated trauma to the feet due to everyday activities.
 nail disorder-1 psoriasis
nail disorder-1 psoriasis
Symptoms
Onychomycosis
- Possible separation of nail from nail bed
- Buildup of white, green, yellow or black debris under the nail
- Discoloured nail bed and foul odour
- Whitening or yellowing of the nail
- Thickened and crumbling nail
- Numbness, tingling or pain
Paronychia
- Redness, pain and swelling
- Abscesses (pus-filled cavities) may form
- Duration is usually acute but chronic paronychia has symptoms lasting more than six weeks
- Symptoms usually occur at the side of the nail fold
- Occasionally the entire horseshoe of skin around the nail is involved
- Green colouration of the nail indicates a Pseudomonas bacteria infection
Ingrown nails
- Redness, swelling and tenderness
- Pain during walking or running
- Corners or sides of nails digging into soft tissue
Other symptoms can indicate a more serious underlying condition. The following are some common signs to watch for when examining your nails:
|
Nail appearance |
Potential cause |
|
White spots on nail |
Mild trauma; may indicate infection |
|
Thin, reddish-brown vertical lines under the nail |
Damage to blood vessels in nail bed |
|
Clear, jelly-filled bubble at nail base |
Cyst that requires removal |
|
Dark spots, streaks |
Injury; if no injury, melanoma (skin cancer) |
|
Pits, ripples, discoloration; crumbling and separation from nail bed |
Psoriatic nails accompanying psoriasis |
|
White nails |
Liver diseases |
|
Half of nail is pink, other half is white |
Kidney diseases |
|
Thick, yellow nails; slow growth |
Lung disease |
|
Nail bed is red |
Heart conditions |
|
Nail bed is pale |
Anemia |
|
Yellow nails, slightly pink at base |
Diabetes |
|
No nail, thick nail, curved nail |
Congenital deformities |
|
Triangular half-moon at base of nail, thumb nails partially absent |
Nail-Patella Syndrome |
|
Concave, spoon-shaped nail |
Plummer-Vinson syndrome |
|
Rough, pitted opaque nail |
Alopecia areata |
|
Horizontal white lines |
Abnormality in blood vessels beneath nail; may point to other conditions such as pellagra, Hodgkin disease, sickle-cell anemia |
Diagnosis and Treatment
Most nail disorders are diagnosed by a doctor through visual examination. In the case of paronychia, laboratory tests may be, but are rarely, required. In the case of onychomycosis, diagnosis is important, as other nail problems can look similar. Analysis is by microscopic examination or culture of the fungus.
Treatment varies depending on the type of nail disorder.
Onychomycosis
Fungal infections can be difficult to cure, and treatment depends on the severity of the symptoms. Some infections will respond to topical antifungal creams, lotions, gels or nail lacquers. However, most fungal nail infections require treatment with oral antifungal drugs (for example, itraconazole, terbinafine or fluconazole). These drugs may improve the condition and completely cure it; however, the infection often recurs when the drugs are discontinued. In some cases, part of the infected nail may need to be removed to allow direct application of a topical antifungal. This treatment is generally effective only in cases where the infection is superficial. The nail will grow back unless the bed is severly injured. Chronic pain may require permanent removal of the nail. Recently laser therapy has been reported as useful in the treatment of onychomycosis, and currently studies are being done to confirm the exact effectiveness of this therapy
Paronychia
Hot compresses and warm soaks can relieve pain and often drain pus. Sometimes, a doctor will make a small cut into the pocket of infection (abscess) to drain it more quickly and then apply an antiseptic. Nail plate removal may be required if the abscess is under a raised nail. If the doctor suspects the infection is spreading or the condition is caused by a fungus, then she or he may prescribe oral antibiotics.
Ingrown nails
If not severe, the foot may be soaked in warm salt or soapy water followed by placement of dry cotton under the corner of the nail. More severe cases require professional removal of ingrown sides and treatment of any infection, as self-treatment could lead to serious infection, particularly if the toe is sore or an open wound is present. A doctor will usually numb the area with anaesthetic and then remove the ingrown section of the nail. The ingrown nail usually doesn’t recur. Chronic cases require professional removal of ingrown nail and its root by chemical, laser or other methods.
*All information on medical treatments on this site is provided as an overview only. For a complete and up-to-date list of side effects, warnings and precautions, read the product’s package insert and consult your doctor or a pharmacist.
**If you are considering an alternative or complementary therapy, discuss it with your doctor first, and always be sure to keep your doctor up to date about any vitamins, supplements, or other forms of alternative treatment you are taking. Like any medication, alternative therapies can interact with other medications/treatments and, in some cases, have side effects of their own. Remember that “natural” does not necessarily mean “safe.”
Coping and Support
Nail disorders generally do not cause as many problems with day-to-day life as other skin conditions. However, ingrown toenails can make walking and running uncomfortable or painful. Paronychia does not normally affect everyday life, but chronic cases may impact some activities. People with the condition may need to break habits such as nail biting or finger sucking to help manage it. Onychomycosis affects people slightly more than the other conditions. It can make walking and typing uncomfortable or even painful. Discoloration and thickening of the nail may be seen as unattractive and therefore embarrassing. In severe cases, the limitations and disfigurement can lead to emotional or psychosocial stress.
Fortunately, people with these conditions can take steps to manage them and prevent them from reccuring. Here are some tips:
Onychomycosis:
- Keep feet clean and dry.
- Avoid nail polish and acrylic nails, which prevent air from reaching the surface.
- Avoid walking barefoot in public showers, pools and locker room areas.
- Change shoes and socks frequently.
- Keep nails clipped short and straight across.
- Wear well-fitting socks and shoes made of breathable materials.
- Disinfect clippers and other instruments used to treat nails.
Paronychia:
- Avoid nail-biting.
- Avoid finger sucking.
- Wear rubber gloves when washing dishes and or performing other activities that require prolonged exposure to water.
- Clean cuts and scrapes promptly to prevent infection.
Ingrown nails:
- After removal of an ingrown nail, follow good nail hygiene practices and choose properly sized footwear.
Neurofibromatosis
Overview: What is Neurofibromatosis?
Neurofibromatosis (NF), is a genetically inherited disorder that is characterized by brown blotches and abnormal growths across the skin and along the nerves. There are seven types of NF, with NF1 (also known as von Recklinghausen disease) being the most common and best-characterized form that has diagnostic skin implications. This disorder affects approximately 1 in 3000 individuals.
Up to 50% of cases of NF1 have been seen in individuals whose parents did not have the disease. This suggests up to half of all individuals with NF1 have a spontaneous mutation in their gene(s). The other half of patients with NF1 have parents that have been affected.
Symptoms
There are a wide range of clinical features associated with NF1, with some features being more present than others. Almost every organ system in the body seems to be involved with NF1 also.
Some of the signs and symptoms of NF1 include:
- Café-au-lait macules (CALMs) are tan to dark brown patches that are haphazardly distributed across the body (except the scalp, palms of the hands, and soles of the feet).
- Neurofibromas, are benign abnormal growths or tumours that can develop on the skin and along the nerves.
- Freckling of the skin that typically cluster in skin folds (e.g., armpit, creases of the legs).
- Lisch nodules, are tan-coloured spots situated on the coloured portion of the eye that looks like small freckles.
- An increased risk of having a learning disability such as autism spectrum disorder
- Seizures
- A head size that is generally larger
- High blood pressure
- Problems in the development of the bones, can cause:
- Abnormal bumps across the limbs that appear to be joints but are not.
- Deformed body parts, including the face.
- A curved spine (also known as scoliosis).
- Bones that are fragile and can break readily.
- A shorter stature for your age.
Diagnosis and Treatment
Diagnosis
In order to be clinically diagnosed with NF1, the individual must exhibit at least two of the following clinical features:
- 6 or more CALMs that are >5 mm in diameter in children before they hit puberty and >15 mm in diameter in individuals after puberty.
- 2 or more neurofibromas of any type
- Freckling in armpit region or in the groin region
- A brain tumour that affects the nerve leaving from the eye, going towards the brain (known as an optic nerve glioma)
- Two or more Lisch nodules
- Abnormal bumps across the limbs
- A first-degree relative who has been diagnosed with NF1
Families who have a child with NF1 and are considering having another child, may perform genetic testing of the fetus to know the likelihood of their next child having NF1. This is known as prenatal testing.
Treatment
The management of patients with NF1 necessitates a multidisciplinary approach. Patients are cared for longitudinally, throughout their lives, as symptoms and complications must be detected and treated as they occur.
The child with NF1 must have regular visits at yearly individuals with the multidisciplinary healthcare team. Certain tests must be performed at each visit. Refer to the table below.
|
Type of Examination |
What the physician will do |
Why this is important |
|
Physical exam (every year) |
Examine the skin for signs of any new abnormal growths. Check for high blood pressure. Measure the height, weight, and head size. Check the arms, legs, and back for any abnormal bone growths or abnormal curvature |
NF1 can change how the body grows and forms. It can cause high blood pressure which can lead to heart disease, and other heart problems. |
|
Eye exam (every year) |
A full eye exam, including visual screening |
NF1 can cause tumours to grow behind the eye which can affect vision |
|
Check for signs of early puberty (every year) |
Look for hair growth under the arms or between the legs. Look for budding breasts (in girls). Look for growth of the penis or testicles (in boys). |
NF1 can cause tumours in the part of the brain that controls the timing of puberty. |
|
Check on learning and memory (every year) |
The child will be assessed for any learning problems, undergo a developmental assessment, and be assessed for signs of ADHD (attention-deficit hyperactivity disorder). |
If the child has any learning problems, it is vital that this is identified at an early stage so they do not fall behind in school. |
|
Review school progress (one the child reaches school age) |
Various tests can identify where learning gaps are, if the child is not learning well in school. |
There are special classes available with tutors that can assist the child |
|
Look for large, abnormal skin growths (each year) |
Patients are questioned as to whether any of the growths hurt more than normal. |
This can suggest that the abnormal growth on the skin is becoming a cancer |
Medications also exist for patients with increase bone fragility. Other bone abnormalities such as scoliosis may require surgical intervention by an orthopedic surgeon. Blood pressure can also be managed through a combination of diet, exercise, and medication.Children that have learning disabilities should obtain academic support if it is available. There are also speech, occupational, and physical therapy available for kids with speech problems, and balance and walking issues. Children with ADHD may require the need of medication to lower their hyperactive states. Medications also exist for individuals with seizures.There are various tumours associated with NF1. There are different treatment options that depend on the tumour type. Tumours on the skin tend not to be removed unless there is a specific need for removal (e.g., pain, bleeding, disfigurement, etc.). Larger tumours may need to be surgically removed. If the tumours have become life-threatening, such as a malignant cancer, then this involves the use of surgery, chemotherapy, and/or radiation as treatment.
Coping and Support
Due to the wide variability in the presentation of NF1, affected individuals may either have mild presentations or more severe presentations that are cosmetically disfiguring and are associated with stigma. The cosmetic appearance of NF1 may amount to an attack on one’s self-image. Moreover, the unpredictable nature of this disease can be a source of anxiety for both NF1 patients and their families. Patients may also have learning disabilities that can hinder their economic status and capacity to cope with the burden of the disease.
Patients should speak with their healthcare providers for support and medical advice.
Resources
If you are living with Neurofibromatosis or know someone who is, you may want to stay up-to-date on the condition as well as current treatments and news.
Our Affiliate Member
There are many organizations specialized in this regard for individuals with NF1, such as:
- Neurofibromatosis, Inc. (www.nfinc.org)
- The Neurofibromatosis Clinics Association (www.nfpittsburgh.org)
- The Children’s Tumor Foundation (www.ctf.org)
- The Neurofibromatosis Association of UK (www.nfauk.org)
- Association de la Neurofibromatose du Québec https://www.anfq.org/index.php/en/ (French only)
Porphyria
Overview: What is Porphyria?
Porphyrias are a collection of rare metabolic disorders that influence how the body assembles a substance called “heme”. Heme is an iron-containing compound within red blood cells. It has many important functions in the body including: making the blood the colour red and it also helps to transfer oxygen throughout the body. Individuals with porphyria have a build-up of chemicals called “porphyrins” that can accumulate within the body and cause symptoms. The prevalence rates of porphyrias vary from 0.5 to 10 per 100,000 individuals. It occurs in all races and in both sexes.
There are approximately 8 separate types of porphyria. A majority of them originate from abnormal genes that are passed down families. However, it is possible to be the first person in your family to develop porphyria. The common variants of porphyria are:
- Porphyria cutanea tarda (PCT)
- Acute intermittent porphyria (AIP)
- Erythropoietic protoporphyria (EPP)
Symptoms
Each of the porphyrias will induce different symptoms. As a whole, these symptoms can be separated into two main types: “acute” and “cutaneous”.
Acute porphyria: Acute porphyrias, such as AIP, will happen in the form of “attacks” that typically last a few days but can also last weeks. A variety of things can cause an attack such as medications, alcohol, infection, and stress. Symptoms tend to be diminished between attacks. The symptoms of the acute attack include:
- Belly pain (the most common symptom)
- Vomiting
- Constipation
- Muscle pain, weakness, or numbness
- Seizures
- Anxiety, confusion, depression
- A fast heart beat
Cutaneous porphyrias
- Fragility, erosions and blisters on the skin (particularly on the face and on the back of the hand)
- Skin pain, swelling, and itching
Some porphyrias can cause symptoms of both acute porphyria and cutaneous porphyria. Moreover, some porphyrias occur in childhood while others will first be observed in adulthood.
Diagnosis and Treatment
Diagnosis
If your physician believes you are exhibiting symptoms of porphyria, you will require testing. This can involve tests of your blood, urine, and/or a sample of your bowel movements. Blood tests include measures of the amount of a chemical in your body known as “PBG”, iron levels, assessment for infection, and assessment for liver disease.
Genetic testing may also be performed to identify if an abnormal gene is the cause of your porphyria. Moreover, genetic testing can help identify if you have a gene that causes an abundance of iron that can be stored within the body.
Treatment
It is important to recognize that porphyria is not are not a common condition. Depending on your physician’s experience, he or she may not know a lot about the condition. This is why it is important the physician educates themselves about it. Furthermore, because each specific porphyria has a slightly varied treatment protocol, it is important for your clinician to know about this.
Each of the porphyrias is treated differently.
- Acute porphyrias: These will be treated with medication so that your body will stop producing the chemicals that are causing your symptoms. Also avoidance of triggering medications.
- Cutaneous porphyrias: The primary method of treating these symptoms is to protect your skin from sun exposure. This includes staying outside of the sun until your porphyrin levels are back to normal. However, if you do need to be outside, use protection such as hats, gloves, sunglasses and sunscreen.
Coping and Support
Coping
Many people with porphyrias wonder if they can still have children, as they may have a genetic condition that can possibly be passed down to their child. The answer is definitely yes, you can still have children. It may help to speak with a genetic counselor and discuss the likelihood of passing your condition down.
Having porphyria can prove challenging to many individuals. Sometimes, the symptoms being experienced may seem bizarre, alarming, and confusing. If it feels as though you are having difficulty coping with the condition, speak with a doctor or nurse or counselor.
Resources
Individuals with porphyria may want to stay up-to-date on the conditions as well as novel treatments and news. The following are websites patients can access to stay well-informed:
Our Affiliate
![]() Canadian Association for Porphyria (www.canadianassociationforporphyria.ca)
Canadian Association for Porphyria (www.canadianassociationforporphyria.ca)
Other Resources:
American Porphyria Foundation (www.porphyriafoundation.org)
Psoriasis
Overview: What is Psoriasis?
The CPSA gratefully acknowledges Nadia Kashetsky, MSc, MD candidate, Memorial University of Newfoundland, and Cheryl F. Rosen, MD, FRCPC, for assistance in the preparation of this report. October 2021.
Psoriasis is a common chronic inflammatory skin disorder causing areas of the skin to become thickened and often covered with silvery scales.1 In individuals with darker skin tones, areas with psoriasis may look purple, dark brown, dark gray, or red as compared to red in individuals with lighter skin tones.2–4
Psoriasis occurs mainly in adults, however children and adolescents can develop psoriasis too.1 Females and males are equally affected, and psoriasis is not contagious or an infection.1 Psoriasis affects between 0.2% to 4.8% of the population.5 There are several types of psoriasis as described below.3
Plaque psoriasis
- The most common type of psoriasis, 80-90% of cases.1
- Skin plaques are usually 1-10cm in diameter but may be larger.
- It can occur at any age but tends to begin in young to middle aged adults.
- The severity varies between individuals and over time from mild, moderate, to severe.
- It may occur in a few small areas or may cover a large part of the body.
- The most commonly affected locations include the back of the elbow, the front of the knee (extensor surfaces), and the lower back.
- Psoriasis may or may not be itchy.
- Plaques of psoriasis may occur on the scalp. Psoriasis does not cause hair loss.
Further anatomical classification of plaque psoriasis6
Inverse psoriasis
- Named “inverse” because the presentation is on the flexor surfaces or skin folds.1
- Can occur in the armpits, groin, genitals, buttocks and under the breasts.
Nail psoriasis
- May cause tiny pits in the nails, brown or salmon-coloured spots, or cause the nails to separate from the nailbed.
- If severe, nails may thicken and crumble.
- Seen in 60-80% of patients with psoriasis.
Palmoplantar psoriasis 3
- Occurs on the palms of the hands and soles of the feet.
- Like other types of psoriasis, the skin can crack, bleed and be painful.
- There is also a variant of palmoplantar psoriasis that results in pus-filled bumps, called palmoplantar pustulosis.
Guttate psoriasis
- A sudden eruption of small scaly papules primarily on the trunk.
- Tends to affect children or young adults.
- May occur after a recent streptococcal infection.
Other Types of Psoriasis
Pustular psoriasis
- May be generalised (spread out over the body) or localised (on smaller, specific areas of the body).
- The generalized type is rare and may be severe with a rapid onset of multiple small pustules (pus-filled bumps) which may join to form larger pustules.
- With generalized pustular psoriasis, people may have fever, chills, malaise, and enlarged lymph nodes.
- Palmoplantar pustulosis is a localised form of pustular psoriasis located on the palms of the hands and soles of the feet.
Erythrodermic psoriasis7
- Rare
- The entire skin surface becomes red (erythematous) and scaly.
- People may have fever, chills, malaise, enlarged lymph nodes, joint pain, and a faster heart rate.
Comorbidities (conditions associated with psoriasis)
Psoriatic arthritis1
- An inflammatory arthritis (joint pain and swelling).
- About 1 in 3 people who have psoriasis will develop psoriatic arthritis.
- Psoriasis develops first in 85% of people, however 15% of people experience arthritis first.
- About 80-90% of people with psoriatic arthritis may have nail involvement
Depression
The prevalence of depression is higher in people with psoriasis.
Obesity, heart disease, diabetes, and metabolic syndrome
There is an increased incidence of these conditions in people with psoriasis.
What is the cause of psoriasis?
The exact cause of psoriasis has not yet been identified. However, psoriasis is thought to develop from a combination of genetic, immune, and environmental factors.1
Genetic Factors
Although there is no genetic test to tell you whether you will develop psoriasis, about 40% of individuals with psoriasis or psoriatic arthritis have family members with the disorder.
Immune Factors
In psoriasis, immune cells produce molecules (Interleukin 23, interleukin 12/23, TNF) that contribute to inflammation. These molecules enter the skin through blood vessels, and cause the outer layer of skin (the epidermis) to become thicker, growing very fast without time to develop correctly, leading to surface scaling. Blood vessels in the middle layer of skin (the dermis), dilate which causes redness.
Environmental Factors
Environmental factors that have been linked to psoriasis include:
- Bacterial and viral infections
- Alcohol
- Certain medications (beta blockers, lithium, antimalarial drugs)
- Smoking
- Trauma
Symptoms
Signs and symptoms of psoriasis may include1:
- Raised areas of skin (plaques) that appear red, purple, brown, or gray depending on the person’s skin colour
- Silvery scales
- Itchiness and/or pain of affected areas may be present
- Pitting, discolouration, or crumbly nails
Diagnosis and Treatment
Diagnosis
Psoriasis is usually diagnosed based on the appearance of the skin lesions (a clinical diagnosis). Sometimes, a skin biopsy may be required to rule out other causes of a rash.1
Treatment
Psoriasis is a chronic (long-lasting, persistent) disorder which may improve or worsen over time. There is no cure at this time. However, treatments may be used very effectively to decrease signs and symptoms.1
There are several types of treatment available for people with psoriasis which include:
Topical medications8
- Topical corticosteroids (creams, ointments or lotions) are recommended for plaque psoriasis. They are recommended as first line for mild psoriasis.9
- Milder steroid creams may be used in the skin folds (where skin rubs together).
- Other topical agents include vitamin D analogs, retinoids, and calcineurin inhibitors that can be used alone or in combination with steroids.8
- Other topical treatments like moisturizers with or without salicylic acid can be used alone or in combination with steroids.
Ultraviolet (UV) Radiation: Phototherapy
- In summer months or on sunny winter vacations, individuals often notice improvement of psoriasis with sun exposure.
- Different types of UV radiation treatment, most commonly narrow band UVB,10 may be available at your dermatologist’s office or at a specialized phototherapy centre. In some places, home phototherapy is available.
- It is important to note that therapeutic phototherapy is different from tanning beds, which are not recommended. Tanning beds emit mostly UVA radiation which is not effective for psoriasis. The use of tanning beds is associated with an increased risk of skin cancer - therapeutic narrowband UVB is not.
Systemic medications (oral medications)13
- Methotrexate may be used to treat moderate to severe psoriasis in adults, including plaque psoriasis, erythroderma, generalized pustular psoriasis, and palmoplantar psoriasis.
- Methotrexate may also be given as an intravenous, intramuscular, or subcutaneous injection.
- Acitretin is an oral retinoid that may be used for moderate to severe psoriasis in adults.
- Apremilast may be used to treat moderate to severe psoriasis in adults.
- Cyclosporine may be used to treat severe psoriasis, and can also be used for erythrodermic, generalized pustular psoriasis, and palmoplantar psoriasis. Cyclosporine is not recommended for longterm use.
Biologics 14
Biologics, which target the individual components of the immune system, work to block the molecules that contribute to inflammation: interleukin 23 (IL-23), interleukin 12/23 (IL-12/23), interleukin 17 (IL-17), and TNF (tumour necrosis factor). They are generally reserved for people who have not responded to other treatments, due to their high cost. However, biologics may have fewer side effects than cyclosporine, methotrexate, and acitretin. They can be very effective as a treatment for moderate to severe psoriasis.
Biologics include:
- TNF-alpha inhibitors (etanercept, infliximab, adalimumab, certolizumab)
- IL-12/IL-23 inhibitors (ustekinumab)
- IL-17 inhibitors (secukinumab, ixekizumab, brodalumab)
- IL-23 inhibitors (guselkumab, risankizumab)
For the treatment of women of child-bearing potential, TNF-alpha inhibitors and IL-12/IL-23 inhibitors have not shown negative maternal-fetal outcomes.15 Data for IL-17 and IL-23 inhibitors is currently limited. All biologics are likely safe during breastfeeding.
Alternative medicines8
Due to lack of evidence or conflicting evidence there are no current recommendations for alternative therapies, including:
- Diet/dietary supplements
- Mind/body interventions (stress reduction, meditation, hypnosis)
- Herbal therapies (Aloe Vera and St. John’s Wort)
- Traditional Chinese Medicine
Treatments available for children with psoriasis include16:
- Calcipotriol ointment with or without topical steroids. 17
- If psoriasis is resistant treatment with creams and ointments narrow band UVB phototherapy may be helpful if it is accessible. Methotrexate may be used when topical treatment and phototherapy have not been successful.
- Etanercept, adalimumab, and ustekinumab are biologics approved in Canada for the treatment of psoriasis in children.18
*All information on medical treatments on this site is provided as an overview only. For a complete list of benefits, side effects, warnings and precautions, read the product’s package insert and consult your doctor or a pharmacist.
**If you are considering an alternative or complementary therapy, discuss it with your doctor first, and always be sure to keep your doctor up to date about any vitamins, supplements, or other forms of alternative treatment you are taking. Like any medication, alternative therapies can interact with other medications/treatments and may have side effects of their own. Remember that “natural” does not necessarily mean “safe.”
Coping and Support
A diagnosis of psoriasis may change how people view themselves and perceive others. It may have a detrimental emotional impact and make people feel confused, overwhelmed, displaced, isolated, misunderstood, fearful of the future, controlled by psoriasis, and challenged by everyday life.
Some tips to take an active role in your psoriasis management by the Canadian Association of Psoriasis Patients include:
- Consider joining support groups, including online or in person support groups.
- Prepare your family and friends by establishing good communication and boundaries.
- Asking your family and friends to learn more about psoriasis.
- Letting your support team know how you are feeling and being clear about your needs.
- Consider greatly reducing your intake of alcohol or even cutting it out altogether.
- Eat a well-balanced diet.
- If you are overweight, losing weight can reduce joint stress on your knees. Losing weight can also help reduce folds of skin on your body where psoriasis can appear. Please talk to your doctor, a registered dietitian, and/or a kinesiologist to discuss safe weight loss practices
- Consider quitting smoking.
- Protect your skin by using gentle products, keeping your skin moisturised, and keeping up with your medications.
The Canadian Association of Psoriasis Patients has developed an excellent resource and guide to living well after receiving a diagnosis of psoriasis titled Living with Psoriasis. For more strategies for coping and support, Living with Psoriasis can be found at: https://www.canadianpsoriasis.ca/index.php/en/psoriasis/living-with-psoriasis
Resources
If you are living with psoriasis or know someone who is, you may want to stay up to date on the condition as well as current treatments and news.
Our Partner Organization
 Canadian Association of Psoriasis Patients
Canadian Association of Psoriasis Patients
Our Affiliate Members
 Canadian Arthritis Patient Alliance
Canadian Arthritis Patient Alliance
Psoriasis Patient Decision Aid
This decision aid has six steps to guide you through the process of choosing which treatment option best suits you: https://www.informed-decisions.org/psoriasispda.php
Magazine articles
 |
 |
The Painting Psoriasis Project
|
Psoriasis: Mild, moderate, severe
|
Rosacea
Overview: What is rosacea?
The information in this section has been gathered from existing peer-reviewed and other literature and has been reviewed by expert dermatologists on the CSPA Medical Advisory Board.
Rosacea is a chronic inflammatory disease that affects the skin on the face and sometimes the eyes. No one knows what causes rosacea, but it may run in families or be the result of an immune system dysfunction caused by a substance called cathelicidin. People with rosacea have an excessive amount of cathelicidin in their skin, which may explain why they react to certain environmental triggers.
Rosacea is not dangerous or contagious and does not scar, but its effects can cause embarrassment or low self-esteem. There are four types of rosacea:
- Erythematotangiectatic rosacea affects the face.
- Papulopustular rosacea affects the face.
- Phymatous rosacea affects the nose.
- Ocular rosacea affects the eyes.
 rosacea-1
rosacea-1  rosacea-2
rosacea-2
Symptoms
Rosacea can range from mild to severe, and every person’s experience is different. Although rosacea can sometimes look similar to acne (and is often misdiagnosed as acne vulgaris or seborrhoeic dermatitis), they are completely different conditions. Unlike acne, rosacea is systemic, meaning it affects the whole body and can cause internal, as well as external, symptoms, which can include:
- Skin redness, usually in the centre of the face, covering the cheeks, nose, forehead and chin (common in erythematotelangiectatic rosacea)
- Dry, thick or scaly skin
- Pimples, which can be inflamed, hard, red or filled with pus (common in papulopustular rosacea)
- Red lines, called telangiectasia, which appear when small blood vessels get larger and show through the skin (common in erythematotelangiectatic rosacea)
- Knobby bumps on the nose and eventual enlargement of the nose due to excess tissue build-up (common in phymatous rosacea)
- Eye inflammation, resulting in swollen eyelids, styes, burning, stinging or irritation and a watery or bloodshot appearance (common in ocular rosacea)
- Vascular dysfunction, such as hypoxemia (an inadequate supply of oxygen to the blood) in the face, extremities and bowels
If you experience any of these symptoms, visit your doctor as soon as possible. Treating rosacea early on is the key to effectively controlling this condition.
Diagnosis and Treatment
The diagnosis for rosacea is based on recognition of its signs and symptoms by a doctor. There is no lab test for this condition.
Although there is no cure for rosacea, a number of treatment options are available to help control it. Treatment for rosacea is typically a long-term process. It can take one to two years to bring the disorder under control, and lifelong treatment is often necessary. However, in some cases the condition resolves quickly and goes into permanent remission.
Lifestyle Changes
The first line of treatment for rosacea is learning to avoid its triggers. Keep a diary of your rosacea flare-ups to help you determine which of the following triggers affect you most:
- Extreme temperatures and temperature changes, including moving from inside to outside
- Strenuous exercise
- Heat from sunlight
- Severe sunburn
- Stress and anxiety
- Fragranced soaps and soap-based cleansers
- Certain food and drinks, including caffeine, spicy foods and foods containing histamines, such as cheese, fermented soy products, vinegar, alcohol and other fermented foods
- Certain medications and topical irritants, such as blood-pressure drugs, microdermabrasion, chemical peels, high doses of isotretinoin, benzoyl peroxide, tretinoin, topical steroids and demodex mites (tiny mites found in the hair follicles)
Treatment Options
Several approaches can relieve rosacea symptoms. Some of the treatments, like laser and light therapy, act by reducing skin thickness and the size of visible blood vessels. For more serious cases of rosacea, one involving papules or pustules, more aggressive anti-inflammatory or antibiotic treatment might be recommended. These treatments will reduce redness by dampening the reaction of your immune system or by killing invading bacteria.
Topical treatments (creams, gels, ointments)
Antibiotic/steroid combinations are used to treat rosacea that affects the eyes. These medications target bacteria and reduce inflammation and immune system activity. To use, apply one or two drops to affected eyes every one or two hours for several days. Following this, apply one or two drops three or four times daily. You should not use this type of drug if you have a viral or fungal infection of the eye, or if you have tuberculosis. These medications may increase pressure within the eyeball; this should be checked regularly if you use these products for more than 10 days.
Laser and light therapies can treat skin thickening on the nose and face, redness, and the dilated blood vessels associated with rosacea. Lasers selectively target excessive tissue and blood vessel lesions while reducing damage to surrounding skin. A health professional will administer laser treatments. Your condition may be resolved after one treatment, but may require several visits, separated by three to eight weeks. Common side effects include bruising and fluid accumulation around the site of treatment.
Metronidazole is a topical anti-inflammatory cream used to treat papules, pustules and erythema of rosacea. The medication is applied to the affected area after washing once in the morning and once in the evening. Metronidazole can irritate the eyes, so apply the cream carefully to the face and avoid the eye area. Tell your doctor if you have a history of blood disorders. Reported side effects include skin sensitivity, burning and itching.
Mild skin cleansers gently remove oil and dirt from the skin without increasing irritation. Although cleansers are not a specific treatment for rosacea, they are included here because good skin hygiene is important for rosacea. To use, cleanse affected and unaffected areas each morning and evening before applying topical medications.
Systemic Treatments
Antibiotics (e.g., tetracyclines, including minocycline and doxycycline) are prescription medications that can improve rosacea. Some antibiotics are approved for rosacea, while others are approved only for use against acne but may be effective in treating rosacea. To use, take the antibiotic pills as prescribed, usually twice a day for at least six months. Prepare for long-term treatment; effects will be evident after one month, but treatment may continue for at least eight months. Side effects include an upset stomach.
Other Treatments
Other medications officially approved for treating other conditions and diseases have been tried in rosacea with variable success. Some medications are approved for rosacea in other countries, but not in Canada. These prescription medications are included here for information only: erythromycin/benzoyl peroxide/tretinoin combination products, beta blockers (e.g., labetalol, propranolol, atenolol), clonidine, isotretinoin, and azelaic acid.
As research continues into rosacea, researchers may be developing new drugs to treat it.
*All information on medical treatments on this site is provided as an overview only. For a complete and up-to-date list of side effects, warnings and precautions, read the product’s package insert and consult your doctor or a pharmacist.
**If you are considering an alternative or complementary therapy, discuss it with your doctor first, and always be sure to keep your doctor up to date about any vitamins, supplements, or other forms of alternative treatment you are taking. Like any medication, alternative therapies can interact with other medications/treatments and, in some cases, have side effects of their own. Remember that “natural” does not necessarily mean “safe.”
Coping and Support
Our facial appearance affects how we feel about ourselves and how we interact with others. Therefore, the noticeable skin changes on the face common in rosacea can have a profound long-term effect on a person’s quality of life by causing low self-esteem, embarrassment, frustration and sadness.
The flushing associated with rosacea can be especially embarrassing since it can be unpredictable and severe, and the permanent reddening of the face can make patients worry that they are perceived as heavy drinkers. Older men, whose noses become bigger and knobby, may feel ashamed and avoid being seen in public. The impact of this disease should not be underestimated by friends and family members.
However, the good news is that the symptoms associated with rosacea typically disappear as the condition is brought under control. Avoiding anything that triggers your rosacea and sticking to the long-term treatment plan prescribed by your doctor are vital strategies for coping with this condition and eventually getting relief from its physical and emotional effects.
That being said, seeking social support can help people manage the emotional aspects of rosacea.
Visit the Acne and Rosacea Society of Canada to get support, information and advice from other people with rosacea.
A Patients Story:

Click here to read Cathy's Story - a nurse who has lived with rosacea for decades.
Resources
If you are living with Rosacea or know someone who is, you may want to stay up-to-date on the condition as well as current treatments and news.
Our Affiliate
Acne and Rosacea Society of Canada ![]()
Other Resources
Acne and Rosacea Society of Canada - offering and help - printable pdf
Rosacea Patient Decision Aid
This decision aid has six steps to guide you through the process of choosing which treatment option best suits you: https://www.informed-decisions.org/rosaceapda.php
Scleroderma
Overview: What is scleroderma?
The information in this section has been gathered from existing peer-reviewed and other literature and has been reviewed by expert dermatologists on the CSPA Medical Advisory Board. (April 2017)
Scleroderma is a chronic hardening and contraction of the skin and connective tissue, either locally or throughout the body. This is a relatively rare autoimmune disease which means that it is a condition in which the body’s immune system attacks its own tissues. It is also known as systemic sclerosis.
In some forms of scleroderma, hard, tight skin is the extent of this irregular collagen over-production process. In other forms, however, the problem goes much deeper, and may severely affect blood vessels and internal organs such as the heart, lungs, and kidneys.
Scleroderma affects women more often than men and most commonly occurs between the ages of 30 and 50. The cause of scleroderma is still unknown but researchers are working hard to make those determinations. It is known that scleroderma involves an overproduction of collagen.
Symptoms
The symptoms of scleroderma vary greatly for each person, and the effects of scleroderma can range from very mild to life threatening. The seriousness severity depends on which parts of the body are affected and the extent to which they are affected. Prompt and accurate diagnosis and treatment may minimize the symptoms of scleroderma and lessen the chance of irreversible damage.
Skin. Nearly everyone who has scleroderma experiences a hardening and tightening of patches of the skin. These patches may be shaped like ovals or somewhat linear; they can be limited to a small area or cover wide areas of the trunk and limbs. The number, location and size of the patches vary by type of scleroderma. Skin can appear shiny because it's so tight, and movement of the affected area may be restricted.
Fingers or toes. One of the earliest signs of scleroderma is an exaggerated response to cold temperatures or emotional distress, which can cause numbness, pain or color changes in the fingers or toes. Called Raynaud's disease, this condition can also occur in people who don't have scleroderma.
Digestive system. In addition to acid reflux, which can damage the section of esophagus nearest the stomach, some people with scleroderma may also have problems absorbing nutrients if their intestinal muscles aren't moving food properly through the intestines.
Heart, lungs or kidneys. Scleroderma can affect the function of the heart, lungs or kidneys to varying degrees. These problems, if left untreated, can become life-threatening.
Diagnosis and Treatment
There is currently no cure for scleroderma however several treatment options exist to mitigate the symptoms of the disease:
- Blood pressure medications that dilate blood vessels may help prevent lung and kidney problems.
- Drugs that suppress the immune system, such as those taken after organ transplants, may help reduce scleroderma symptoms.
- Medications can relieve symptoms of acid reflux.
- Antibiotic ointment, cleaning and protection from the cold may help prevent infection of fingertip ulcers caused by Raynaud's disease.
- Regular influenza and pneumonia vaccinations can help protect lungs that have been damaged by scleroderma.
- If over-the-counter pain relievers don't help enough, you can ask your doctor about stronger medications.
Surgery is a last resort to treat complications from scleroderma.
Coping and Support
Here are some lifestyle and home remedies to help manage symptoms:
- Stay active. Exercise keeps your body flexible, improves circulation and relieves stiffness. Range-of-motion exercises can help keep your skin and joints flexible.
- Don't smoke. Nicotine causes blood vessels to contract, making Raynaud's disease worse. Smoking can also cause permanent narrowing of your blood vessels. Quitting smoking is difficult — ask your doctor for help.
- Manage heartburn. Avoid foods that give you heartburn or gas. Also, avoid late-night meals. Elevate the head of your bed to keep stomach acid from backing up into your esophagus (reflux) as you sleep. Antacids may help relieve symptoms.
- Protect yourself from the cold. Wear warm mittens for protection anytime your hands are exposed to cold — even when you reach into a freezer. When you're outside in the cold, cover your face and head and wear layers of warm clothing.
As is true with other chronic diseases, living with scleroderma can place you on a roller coaster of emotions. Here are some suggestions to help you even out the ups and downs:
- Maintain normal daily activities as best as you can.
- Pace yourself and be sure to get the rest that you need.
- Stay connected with friends and family.
- Continue to pursue hobbies that you enjoy and are able to do.
Keep in mind that your physical health can have a direct impact on your mental health. Denial, anger and frustration are common with chronic illnesses.
(Source: Mayo Clinic, Scleroderma Society of Canada)
Resources
If you are living with Scleroderma or know someone who is, you may want to stay up-to-date on the condition as well as current treatments and news.
Our Affiliate Members
![]() Scleroderma Society of Ontario
Scleroderma Society of Ontario
Other Resources
Shingles/Herpes Zoster
Overview: What is Shingles/Herpes Zoster?
The information in this section has been gathered from existing peer-reviewed and other literature
Herpes zoster (HZ) or shingles, is a localized, blistering, painful rash that is caused by reactivation of the varicella zoster virus (VZV). Nearly 1 in 3 Canadians develops shingles in their lifetime.
VZV causes a primary infection (called varicella or chicken pox) and reactivation of latent infection (called HZ or shingles). Anyone who has previously had chicken pox can develop shingles. After chicken pox clears, the VZV hides in some nerve cells of the spine or brain indefinitely. The virus can get reactivated at this site in the nerve when the immune system gets weaker, such as through aging or among those taking immunosuppressive medications. Older age is the main risk factor for shingles as over two-thirds of cases occur among individuals over 50 years of age.
VZV can be spread from a person with active shingles to an unimmunized individual who has never had chickenpox, however you cannot catch shingles directly. The transmission of virus can occur by direct contact with localized skin lesions, or by the airborne route.

Symptoms
The first sign of shingles is pain along one of the sensory nerves where the virus is active. The patient may also feel unwell with fever and headache. Occasionally, lymph nodes, small bean shaped structures under the skin, may swell up near the affected area as they are fighting infection.
Within one to three days of having pain, a red, raised, blistering rash starts in the region of the pain. There are often grouped small blisters known as vesicles, which can ooze. New lesions may continue to erupt for several days. As time progresses, the lesions crust and scab as they heal. As the VZV infection hides in the nerve cells of the spine, the rash is commonly limited to the area of the skin supplied by that nerve, rarely crossing the midline to the other side of the body. Nerve supply regions that are commonly affected include the face, neck, chest and abdomen, but any site can be affected. Occasionally, blisters can occur inside mouth, ears, around the eyes or in the genital area.
Pain and other symptoms usually subside as the rash disappears. The recovery is usually completed in 2-3 weeks in children and young adults, and within 3-4 weeks in older patients.
After resolution of the rash, the most debilitating and frequent complication of shingles is post-herpetic neuralgia, which is defined as persistent or recurrence of pain in the same area as the initial rash, more than one month after the infection. Individuals may experience a continuous burning sensation, increased sensitivity or shooting pain. The overlying skin is often numb or sensitive to touch and may result in itch. Other potential complications of shingles include eye infection, central nervous system infection, nerve palsies, neuromuscular disease including Guillain-Barré Syndrome, pneumonia, hepatitis and secondary bacterial infections. The risk of dying of shingles is very low, but post-herpetic neuralgia can be extremely uncomfortable.
Diagnosis and Treatment
Diagnosis
Among people with normal immunity, the diagnosis of shingles is based on clinical presentation – the lesions are unilateral, usually painful with a vesicular eruption in a well-defined nerve distribution pattern (dermatomal). Confirmatory laboratory tests are very seldom needed.
Among people with weakened immunity, shingles may present with unusually severe lesions, and multiple sites involved. They may also spread to the blood and internal organs.
VZV can be cultured from active lesions, but it is not possible in the laboratory to distinguish chickenpox from shingles, as they are the same virus.
Treatment
Mild cases of shingles do not require therapy and resolve fairly quickly. However, there is a tendency to treat most cases as long as the treatment is started very early, within 3 days of the onset of blisters.
As shingles is a viral infection, the mainstay treatment is high dose oral antivirals such as acyclovir, valacyclovir or famciclovir. These are usually given for one week and can shorten the duration of the disease. Severe cases may warrant intravenous acyclovir.
In addition to antiviral therapy, patients are advised to rest, get pain relief from over the counter medications and apply protective ointment such as petroleum jelly to the rash. Occasionally, oral antibiotics may be prescribed by your doctor for any secondary bacterial infections that may develop.
How can shingles be prevented?
Vaccines do not completely prevent shingles but do reduce the risk of contracting it; they may also reduce the likelihood of post-herpetic neuralgia.
Currently, two different shingles vaccines are approved for use in Canada. They are called Zostavax II and Shingrix. Zostavax II is a live vaccine whilst Shingrix is not. Health Canada recommends Shingrix for all individuals ≥50 years of age who do not have a history of allergic reaction after vaccines, or immediate hypersensitivity to any component of the vaccine or its container. Shingrix can be administered regardless of whether the person has a history of chicken pox.
When Shingrix is contraindicated, Zostavax II can be offered. Being a live vaccine, Zostavax II is contraindicated in those who have immunocompromised states, are on immunosuppressive medication, have untreated tuberculosis or are pregnant.
Shingrix requires two doses 2 to 6 months apart. Zostavax II requires one dose. There is no recommendation for a booster dose.
Coping and Support
Coping with shingles
- Remember that most cases of shingles resolve within a few weeks without any serious complications
- Simple measures like acetaminophen and cold compresses are often sufficient to relieve symptoms in the short term
- The contagiousness of shingles is quite low
- It might be necessary to miss work or school for several days, but long absences are unusual
- Rest and relaxation can help
SJS/TEN
Overview: What is SJS and TEN?
Overview: What is Stevens-Johnson Syndrome and Toxic Epidermal Necrolysis
Stevens-Johnson Syndrome (SJS) and Toxic Epidermal Necrolysis (TEN) are two rare, but very problematic and life-threatening skin conditions. SJS and TEN cause the skin to become red and purple, cause tenderness, and cause the skin to peel away from the body. These diseases affect not only the skin on the external surface of the body, but also affect the moist lining of the mouth, nose, eyes, genitalia, and other body parts. TEN is a more severe form of SJS. The extent of skin involvement (body surface area – BSA) classifies a patient into one of three groups:
- SJS: <10% of BSA
- SJS-TEN overlap: 10-30% of BSA
- TEN: >30% of BSA
SJS and TEN have an annual incidence of 1.2–6 and 0.4–1.2 per million persons, respectively. Women are more affected than men, with a ratio of 1.5:1. The incidence of SJS/TEN will rise with age also. Patients that are more high risk are those that have HIV and patients with brain tumours that are undergoing treatment with radiotherapy and also are receiving anti-seizure medications at the same time.
SJS/TEN is mostly caused by an extremely rare side effect of medicine. Development of SJS/TEN cannot be predicted, but as mentioned previously, the likelihood rises slightly if the patient has an HIV infection. It can also occur in children with different infections.
There are over 100 drugs that have been associated with SJS/TEN. The likelihood that a patient will develop SJS/TEN from these medications is highest during the first 8 to 10 weeks of taking the medication. The following medications are most likely to cause SJS/TEN:
- Medication used to treat infections, such as:
- Trimethoprim-sulfamethoxazole
- Nevirapine: an HIV medication, not commonly used.
- Medication that is used to treat gout:
- Allopurinol
- Medication used to prevent seizures, known as “anti-epileptic drugs”
- Carbamazepine
- Phenytoin
- Lamotrigine
- Phenobarbital
- Medication used to treat pain, known as “non-steroidal anti-inflammatory agents”, also known as “NSAIDs”:
- Meloxicam
- Piroxicam
- Tenoxicam
Symptoms
The symptoms of SJS/TEN affect the skin primarily. Typically, 1-3 days before the presence of skin symptoms there are several notable signs observed, including:
- Fever (typically greater than 390C).
- Flu-like illness
- Itching or burning of the eyes
- Pain upon swallowing
- Joint pain
- Cough
Symptoms that develop later on in SJS/TEN may include:
- Spots or patches of red skin that are tender to the touch. These patches can appear darker in colour in the middle, and lighter on the edges of the patch.
- Bruises on the skin can have a blister above.
- The skin of patients can blister or peel. This typically occurs on the chest, face, palms of hands, or soles of feet. These blisters can peel easily and with slight pressure of the thumb can be displaced to the side. Thus, patients must be handled with extreme care.
- On the lips, the moist inside lining of the mouth, eyes, vagina, penis, lungs and other areas, there are sores, swelling and crusting. This can cause:
- Watering of the eyes, red eye, and extreme light sensitivity.
- Different parts of the eye sticking to one another.
- Burning sensation with urinating, or difficulty urinating.
- Difficulty with breathing as lungs can build up with fluid, or lung infections can occur.
Diagnosis and Treatment
Diagnosis
The diagnosis of SJS/TEN is made based upon the clinical features described above. If you or anyone you know has developed these symptoms, go to the emergency room right away or call for an ambulance.
If you are suspected of having SJS/TEN, the physician would want to know the drug that has caused the symptoms, so that it can be withdrawn as early as possible, and improve the prognosis. It’s also important that this drug is identified so that the patient is not re-exposed in the future. At their disposal, physicians will have a tool to use called the algorithm of drug causality for epidermal necrolysis (ALDEN). For patients taking multiple medications, this tool is used to determine the likelihood of which of the many drugs the patient is on is the offending one.
Physicians may also perform a routine skin biopsy so that they can examine it under a type of lighting called immunofluorescence and confirm that they have the correct diagnosis of SJS/TEN, and not a mimic of SJS/TEN. The doctor may also order other tests, such as bacterial and fungal cultures, and blood tests to determine if there are any signs of infection.
Treatment
Patients with SJS/TEN are treated in the hospital, and this typically lasts 2 to 4 weeks. The management of patients requires a multidisciplinary team of healthcare providers including doctors (intensivist, specialized dermatologist, and plastic surgeon), nurses, and other professionals. The following steps will be taken by the treatment team:
- Prompt discontinuation of the offending medication that caused SJS/TEN (if it was induced by medication).
- Appropriate wound care: the skin will be kept as healthy and clean as possible by removing dead skin and applying different kinds of dressings.
- Patients will be intubated with a feeding tube to obtain proper nutrition and fluids. A great deal of fluid is lost in patients with SJS/TEN, and it is necessary to replace this fluid.
- Physicians can provide strong pain medication to help alleviate the intensity of the pain associated with this skin infection.
- Patients are at very high risk of developing an infection, and it is imperative that physicians help in reducing your risk of developing them. Sterile handling is essential in patients with SJS. Antiseptic solutions can be prepared before dressing any wounds. Antibiotics can be given to treat any infections as well.
- Medication can also be given to reduce inflammation.
Coping and Support
SJS/TEN is found to have a persisting impact on patients' lives, both physically and psychologically, including many unanswered questions and concerns. Patients are at increased risk of depression and post-traumatic stress disorder following admission to the intensive care unit. Many patients are unable to work following hospital discharge, and others may require modification to their work environment.
Patients are encouraged to speak to their healthcare provider regarding SJS/TEN should they require more education on the disease.
Resources
If you are living with SJS/TEN, or know someone who is, you may want to stay up-to-date on the condition as well as current treatments and news.
Our Affiliate Member:
 Stevens-Johnson Syndrome Canada
Stevens-Johnson Syndrome Canada
Sun Damage
Overview: What is sun damage and premature skin aging?
The information in this section has been gathered from existing peer-reviewed and other literature and has been reviewed by expert dermatologists on the CSPA Medical Advisory Board.
Skin ages prematurely from prolonged exposure to ultraviolet (UV) radiation from the sun. In fact, UV radiation is the most important factor in premature skin aging, accounting for about 90 percent of the symptoms.
 sundamage-1
sundamage-1
Damage to the skin caused by excessive sun exposure can be:
- Acute, which can be caused by as little as a few hours exposure, producing the reddened, blistered skin commonly known as sunburn
- Chronic, which is caused by the accumulated exposure of skin to the sun throughout a person’s life, producing photodamage or photoaging and, in more and more cases, worrying pre-cancerous lesions and skin cancers. This chronic damage can occur even from sun exposure that does not induce sunburn.
UV radiation comes in two forms:
- UVA radiation
- UVB radiation is the most harmful type of ultraviolet radiation. It is nearly 1000 times more capable of inducing sunburn than UVA rays. UVB tends to peak in intensity between 11 a.m. and 4 p.m. in summer. While UVB does not penetrate deep into the skin, it can damage the DNA at the heart of skin cells and is one of the foremost causes of skin cancer. UV radiation also irradiates white blood cells, thereby suppressing the body’s immunity. It takes about two weeks for your immune system to recover after a sunburn.
Sun damage is permanent and irreversible. It also accumulates, so that damage to the skin from one year is added to the damage done in previous years. This explains why the elderly are more prone to skin cancer. Fair-haired, pale-skinned people are the most vulnerable to sun damage, but all skin types are at risk. Other factors that contribute to premature skin aging include:
- Smoking
- Tanning studios (there is no such thing as a “safe” tan)
- Pollution (particularly ozone) and
- Rapid weight loss.
In addition, sun exposure has been linked to these conditions:
Actinic Keratosis (AK): AK is strongly associated with UV exposure and sun damage, and it is the most common form of precancerous skin lesions (pre-malignant) in humans. The lesions can develop into squamous cell carcinoma (Skin Cancer: Non-Melanoma section), a form of non-melanoma skin cancer that may ultimately lead to death. Risk factors include being over the age of 40, being exposed to high levels of UV radiation, and having a weak immune system.Basal Cell Carcinoma (BCC): BCC is the most frequent type of human cancer. It is associated with chronic sun exposure and occurs mostly on exposed areas such as the face and the trunk. To read more on BCC, visit the Skin Cancer: Non-melanoma section.
Squamous Cell Carcinoma(SCC) SCC is a skin cancer caused by excessive cumulative (long term) sun exposure. These are usually scaly, non-healing spots on sun-exposed areas of the skin. To read more on SCC visit the Skin Cancer: Non-Melanoma section.
Melanoma: The most dangerous form of skin cancer, melanoma is a cancer of the pigment-producing cells of the skin. It can appear as a dark tumour, although this is not always necessary. If untreated, it can spread to lymph nodes and other bodily organs, and it can cause death.
Symptoms
Sun damage and its consequence, premature skin aging, present a variety of symptoms:
- Fine and coarse wrinkles
- Roughness
- Dry, scaly skin
- Laxity or looseness of skin
- Patchy or mottled darker patches of increased pigmentation
- A leathery texture around the back of the neck and coarseness with deep lines
- Thickened layer in the upper dermis known as solar elastosis (chicken skin)
- Lower immunity against infection
- Aging skin disorders
- Cancer
Looking Deeper
As you age, your skin cells divide more slowly and the dermis thins. Fat cells underneath the dermis begin to atrophy, or grow smaller. The underlying network of elastin and collagen fibres, which provides the building blocks for the surface layers, loosens and unravels. The skin loses its elasticity and, when pressed, no longer springs back to its initial position; instead, it sags and forms furrows or wrinkle lines. The skin’s ability to hold moisture also diminishes. The sweat and oil-secreting glands atrophy, depriving the skin of their protective water-lipid emulsions, so that the skin becomes dry and scaly. The ability of the skin to repair itself also diminishes with aging, so wounds are slower to heal. Frown lines (between the eyebrows) and crow’s feet (lines radiating from the corners of the eyes) appear as a result of ongoing small muscle contractions. Characteristic facial expressions also form lines, helping create jowls and drooping eyelids.
Sunburn symptoms include:
- Pink or red colour on the skin
- Tender-feeling skin
- Itchy blisters
- Pain and irritation in the eye from overexposure to UV rays
- Dehydration or fever in severe cases
Actinic keratosis typically appears as barely visible spots or as thick, scaly and sometimes crusty patches of skin. Some AK spots can look like regular skin, but feel like sandpaper. Other symptoms may include:
- Visible spots that may range between a few millimetres up to 2 cm or more in diameter
- Skin discoloration, which may include dark, light, pink or red colours
Diagnosis and Treatment
Prévention
Protéger votre peau contre l’exposition solaire est la meilleure stratégie. Utilisez l’une ou toutes les stratégies suivantes pour vos enfants et vous-même (il n’est jamais trop tard) :
- Porter des vêtements appropriés, incluant un chapeau.
- Porter des lunettes offrant une protection adéquate contre les rayons UV. Choisissez toujours des lunettes de soleil qui bloquent 99-100 pour cent des rayons UV. Certaines étiquettes indiquent « absorption UV jusqu’à 400 nm », équivalant à une « protection à 100 pour cent » contre les rayons UV. Il a été démontré que les rayons UV nocifs pouvaient pénétrer sur les côtés, en haut et en bas de la monture; pour assurer une meilleure protection, choisir une monture enveloppante qui couvre mieux le contour des yeux.
- Appliquer un écran ou une crème solaire, même par temps nuageux ou brumeux. Quinze minutes avant d’aller au soleil et toutes les heures si vous vous baignez ou transpirez, appliquez-le généreusement sur toutes les parties du corps qui pourraient être exposées incluant les oreilles, la nuque, le dos des mains et les parties chauves du crâne.
Cherchons plus loins
Le facteur de protection solaire (FPS) est la mesure utilisée pour calculer l’efficacité protectrice d’un écran solaire. L’indice FPS réel multiplié par 10 vous donne la durée de protection contre les rayons du soleil. Vous devriez utiliser un écran solaire ayant un FPS d’au moins 30 et qui offre un large spectre de protection. Si vous ne pouvez éviter l’exposition prolongée ou intense au soleil (par exemple, si vous travaillez à l’extérieur) et/ou avez le teint pâle et une peau sensible aux rayons UV, un FPS 60 est sans doute préférable. N’oubliez pas que l’indice FPS sur l’étiquette n’est valable que si vous appliquez la crème solaire en quantité suffisante. Les études ont démontré que les personnes appliquent en moyenne 25 à 50 pour cent seulement de la quantité de crème solaire nécessaire pour obtenir la protection indiquée sur l’étiquette.
L’indice FPS sur le contenant de lotion solaire fait uniquement référence au niveau de protection UVB. Plusieurs écrans solaires n’offrent pas la protection à large spectre (UVA et UVB). Pour évaluer le niveau de protection UVA de votre écran solaire, il faut que les ingrédients actifs suivants soient inscrits dans la liste : l’oxyde de zinc, le dioxyde de titanium ou l’avobenzone (qui pourrait être listé sous Parsol 1789 ou Butyle Methoxydibenzoylmethane). Si l’un de ces ingrédients actifs ne fait pas partie de la liste, mais est seulement inscrit dans « autres ingrédients », vous ne recevez pas une protection adéquate et exposez votre peau aux dangers des rayons solaires.
Les traitements
Les coups de soleil
Même si vous n’êtes plus directement exposé au soleil, un coup de soleil continue son œuvre destructive de 12 à 24 heures après la brûlure initiale. Un coup de soleil léger guérira en quelques jours, mais une brûlure sévère avec des cloques peut prendre beaucoup plus de temps à guérir et être très douloureuse. De plus, en pelant vous perdez plusieurs couches cutanées. Bien que les dommages induits par une exposition prolongée au soleil soient irréversibles, certains remèdes peuvent aider :
- Refroidir la partie brûlée du corps sous l’eau froide.
- Prenez de l’aspirine dès que vous êtes conscient d’avoir un coup de soleil.
- Appliquez des lotions rafraichissantes, des cataplasmes et des compresses humides pour réduire l’inflammation (éviter les crèmes/onguents qui retiennent la chaleur au lieu de la dissiper)
La Kératose actinique
Les traitements incluent :
- Le traitement direct de la lésion : enlèvement d’une lésion cutanée unique en utilisant des procédés comme la cryothérapie (par le gel).
- Traitement dirigé sur une surface : traitement de la zone de la peau affectée par la kératose actinique en utilisant des crèmes ou des gels d’application topique, ou encore une thérapie photodynamique.
Les médicaments
Une variété de médicaments est disponible sur ordonnance pour améliorer l’apparence de la peau, incluant :
- La trétinoïne qui est un dérivé de la vitamine A et agit au niveau cellulaire. Des études suggèrent que la trétinoïne en application topique stimule la production de collagène pour améliorer la structure cutanée. La trétinoïne est également utilisée pour diminuer les ridules et les rides, atténuer les taches brunes et améliorer la texture de la peau dans son ensemble.
Les procédures cosmétiques
Une gamme de procédés et de traitements peuvent améliorer, sur certaines zones précises, l’apparence de la peau :
- La blépharoplastie est une intervention chirurgicale qui vise à resserrer la peau et à enlever l’excès de tissus cutanés et graisseux de la région oculaire, redonnant à la peau son apparence de jeunesse. L’intervention peut être combinée à d’autres chirurgies plastiques tel un lifting frontal.
- La toxine botulique A est une toxine puissante dérivée d’une bactérie et doit être utilisée avec la plus grande précaution. Elle vise à atténuer le relief et la profondeur des rides entre les sourcils. Ses effets durent environ quatre mois.
- D’autres interventions incluent le rajeunissement médical ou chirurgical, le peeling chimique, le renforcement des tissus mous, les injections de fillers, la dermabrasion, le relissage electro chirurgical de la peau, les traitements laser non ablatifs et autres sources de lumière non-laser.
En plus des traitements ci-dessus, les chercheurs explorent de nouveaux médicaments pour traiter la peau. Pour vous renseigner sur les recherches en cours au Canada, visitez notre page d’essais cliniques [link to ACPD essais cliniques page].
*Toute l’information de ce site concernant les traitements médicaux est offerte à titre d’aperçu seulement. Pour avoir la liste complète et à jour des effets secondaires, des avertissements, des précautions à prendre, lisez le feuillet qui se trouve dans l’emballage du produit et consultez votre médecin ou un pharmacien.
**Si vous envisagez une thérapie alternative ou complémentaire, discutez-en avec votre médecin d’abord; tenez votre médecin informé de toutes les vitamines, les suppléments ou autre forme de traitement alternatif que vous suivez. Comme tous les médicaments, les thérapies alternatives peuvent interagir avec les autres traitements et, dans certains cas, avoir leurs propres effets secondaires. Souvenez-vous que « naturel » ne veut pas nécessairement dire « inoffensif ».
Coping and Support
Since the skin of the face and the hands is likely to get the greatest exposure to the sun and UV radiation throughout a lifetime, the most significant and evident aging is typically seen there. Unfortunately, these are also the areas most visible to other people and often most closely linked to how we feel about ourselves. Our culture is youth-oriented, and many people hope to keep their youthful looks for as long as possible.
Everyone is different, of course, and while some people easily accept the aging in their skin, others may go to extraordinary lengths to fight it. For this latter group, the impact of aging skin can be profound, affecting their well-being, self-esteem and enjoyment of social events.
The best thing you can do to manage skin aging and control sun damage is to protect your skin from the sun and its UV radiation. The second best thing is not to smoke. Other strategies include:
- Getting plenty of sleep
- Avoiding stress and, when stressed, taking steps to reduce it
Unwanted Facial hair
Overview: What is Unwanted Facial hair?
The amount of body hair you have is largely determined by your genetic makeup and varies widely among women. Usually, a woman will only grow fine hair (peach fuzz) on her lips, chin, chest, abdomen, or back. However, when women grow coarse, dark hairs in these areas, typical of male hair growth, this is a sign of a common yet frustrating condition called hirsutism (HER-soot-iz-um).
While hirsutism can present itself in many areas of the body, this information guide focuses specifically in equipping women with the knowledge to tackle hirsutism on the face or neck also known as unwanted Facial Hair (UFH).
UFH is a medical condition that causes too much hair to grow on a woman’s face and neck. It typically begins to develop during puberty, however, an inherited tendency, hormonal imbalance, or various medications can cause it to appear at any age. Sometimes, the cause remains unknown (idiopathic hirsutism). Regardless of the cause, excess hair, especially on the face, can be a source of great distress for most women, leading to anxiety, depression and reduced quality of life.
There are, however, various strategies to help you effectively manage your UFH. Once a medical diagnosis of UFH is made, you and your physician can explore the treatment options available to you. It is, however, important your physician first rule out any underlying medical conditions.
What are the causes of unwanted facial hair?
Unwanted Facial Hair (UFH) growth in women can be caused by a number of issues. Most commonly, these issues are related to either a hormonal imbalance or the impact of various medications. Sometimes, however, the cause remains unknown (idiopathic hirsutism).
Hormonal Imbalance
All women normally produce low levels of male hormones (androgens). Unwanted Facial Hair (UFH) growth in women may occur when the body makes too much male hormone. Conditions that can cause high androgen levels include:
Polycystic Ovary Syndrome (POS)
POS is one of the most common identifiable causes of hirsutism. This condition is caused by an imbalance of sex hormone levels in a woman’s body that may result in irregular periods, acne, obesity, infertility and sometimes multiple cysts on the ovaries.
Cushing’s Syndrome
This is a condition that occurs when your body is exposed to high levels of the hormone cortisol, a steroid hormone involved in your body’s response to stress. It can develop when your adrenal glands – small hormone secreting glands located just above your kidneys – make too much cortisol, or it can occur from taking cortisol-like medications over a long period of time.
Increased cortisol levels disrupt the balance of sex hormones in your body, which can result in UFH.
Congenital adrenal hyperplasia
This inherited condition is characterized by abnormal production of steroid hormones, including cortisol and androgen, by your adrenal glands.
Menopause
As hormone levels, and even weight, change during and after menopause, some women may find they develop UFH.
Other rare conditions
Rarely, tumours in the ovaries or adrenal gland, formed when abnormal cells grow out of control and clump together may cause UFH.
Medication
Some medications can cause UFH. These medicines include hormones, anabolic steroids and some immunosuppressive drugs.
Idiopathic
Sometimes, there is just no identifiable cause. Excessive facial hair growth in women with normal androgen levels, regular menstrual periods and no other underlying conditions is called idiopathic hirsutism. This occurs more frequently in certain ethnic populations, such as women of Mediterranean, Middle Eastern and South Asian ancestry.
Symptoms
The major sign of Unwanted Facial Hair (UFH) is thick, dark hair appearing on a woman’s face. This hair is typically coarse and pigmented and is different from the hair that some women have on their upper lip, chin, breasts or stomach, or the fine ‘baby’ hair all over their body.
While stray hairs on your face and neck may be not a cause for concern, your doctor can help you understand when UFH is a result of an underlying medical condition.
It is important to pay attention to the development of other signs and symptoms in addition to UFH. Here are a few simple questions that may help you determine whether you are experiencing symptoms that require you to seek medical advice.
Answer ‘yes’ or ‘no’ to the following questions:
• Do you notice rapidly growing, unwanted hair on places such as your upper lip, cheeks, chin, neck, mid-chest, inner thighs, abdomen, or low back?
• Do you notice unwanted hair growth associated with irregular menstrual periods?
• Are you experiencing hot flashes?
• Do you notice an increase in the amount of acne on your face or body?
• Do you suspect there are physical issues affecting your fertility or limiting your ability to conceive?
• Do you notice any unwanted hair growth that appears to be worsened from a medication?
If you answered ‘yes’ to any of the above questions, make sure to see your healthcare professional to discuss your symptoms so that you can be properly diagnosed, rule out any other underlying medical conditions, and help you to decide the best treatment approach for you.
A number of healthcare professionals may be involved in the diagnosis, treatment and management of Unwanted Facial Hair (UFH), including:
• General practitioners/family doctor
• Dermatologists
• Gynecologists
• Endocrinologists
In order for your doctor to make a diagnosis of UFH you will first need to discuss your medical history. Your doctor may ask you about your menstrual cycles, the time of onset of your symptoms, whether you're taking any medications and whether you have a family history of certain conditions. Your doctor is likely to:
1. Perform a physical exam. Your doctor will examine your face. He or she may also conduct a physical examination to check for other signs of androgen excess and for conditions that can result in a hormonal imbalance.
2. Order blood tests. Tests that measure the amount of certain hormones in your blood, including testosterone, may help determine whether your UFH is caused by elevated androgen levels.
3. Further testing. The extent of further testing you'll undergo depends on the severity of your UFH and any other associated symptoms. If androgen levels in your blood are elevated, you may undergo imaging tests. These may include:
• Ultrasound. This imaging test uses high-frequency sound waves to produce pictures of your body's internal structures. An ultrasound of the ovaries or adrenal glands may be performed to check for tumours or cysts.
• Computerized tomography (CT) scan. A CT scan is a type of X-ray test that provides cross-sectional images of your internal organs. A CT scan of your body may be used to evaluate the adrenal glands.
Diagnosis and Treatment
Remember that before starting any treatment regime it is important to first rule out any underlying medical condition. If you are experiencing a rapid increase or sudden onset of facial hair growth, and signs of increased male characteristics, make sure to first see your physician.
Prevention
While Unwanted Facial Hair (UFH) generally isn't preventable and tends to be a long-term issue, a logical starting point is to determine if there are ways to control it. If you are overweight, losing weight will be key to reducing the amount of hormones in your body that are associated with increased facial hair growth.
Treatment
There are numerous ways to remove or treat UFH. Available options can vary in effectiveness, degree of discomfort and cost. Treatment for UFH most often involves a combination of hair removal methods and medications. Therefore, a solid understanding of the various pros and cons of each treatment is a worthwhile exercise as part of your decision-making process. This guide will provide you with an overview of the various treatments available by grouping them into the following categories:
1. Hair Removal Methods
2. Prescription Therapy
Hair removal methods to deal with Unwanted Facial Hair (UFH) include depilatories, which remove hair above the surface of the skin and epilatories, which remove the entire hair including the part below the skin. Here are some examples:
Depilatories:
- Shaving. Shaving is quick and inexpensive, but it needs to be repeated regularly since it removes the hair only down to the surface of your skin.
- Chemical depilatories. Generally available as gels, lotions or creams that you spread on your face, chemical depilatories work by breaking down the protein structure of the hair shaft. Some people are allergic to the chemicals used in depilatories.
- Bleaching. Instead of removing UFH, some women use bleaching agents. Bleaching removes the hair colour, making the hair less visible against some skin tones but potentially more noticeable on darker skin. Bleaching may cause skin irritation, so test the bleach on a small area first.
Epilatories:
- Plucking. Also referred to as tweezing, plucking is a good method to remove a few stray hairs, but is not useful for removing a large area of hair. While plucking may hurt a little and doesn't last forever, it is the most common method women use to get rid of UFH.
- Waxing. Waxing involves applying warm wax on your skin where the unwanted hair grows. Once the wax hardens, it's pulled back from your skin against the direction of hair growth, removing hair. Waxing may sting temporarily and sometimes causes skin irritation and redness. Results usually last a few weeks.
- Threading. This is an ancient method of hair removal originating in the Eastern world. Practitioners use a pure, thin, twisted cotton thread which they roll over areas of unwanted hair, plucking the hair at the follicle level. Unlike tweezing, where single hairs are pulled out one at a time, threading can remove an entire row of hair, resulting in a straighter line. As a larger area of hair is removed at once, however, it can be relatively painful.
- Sugaring. This is used in much the same way as traditional waxing for removing UFH although the ingredients used are few in number and all-natural, typically consisting of sugar, lemon and water. Proponents of sugaring say that it can be done more frequently than waxing with the same benefits and that it causes less skin irritation, among other benefits.
- Home electrolysis. These tools work by applying an electric current through a pair of tweezers. They are good for small areas, and are quick but can be painful. Results may last for many weeks or months. These kits can be costly and may produce skin discoloration.
Other facial hair removal treatments can offer numerous advantages and, although they tend to be expensive, their popularity has made them more widely available with many estheticians and spas. The risk is that the level of expertise and competence of the practitioner is sometimes questionable. Not all laser treatments need to be performed by a doctor but it is advisable that the treatment be administered in a facility when there is a doctor present on-site to supervise the therapy and to ensure that any adverse effects are properly dealt with. The most common facial hair removal therapies include:
- Electrolysis. This type of therapy involves inserting a tiny needle into each hair follicle and emitting a pulse of electric current to damage and eventually destroy the follicle. Electrolysis results in permanent hair removal, but the procedure can be painful. Some numbing creams may be spread on your skin to reduce this discomfort. Side effects include lightening or darkening of the treated skin and, rarely, scarring. As one hair is treated at a time it is a very slow process that requires many repeat treatments. It is best used for small areas.
- Laser Therapy. Laser therapy is a procedure in which a beam of highly concentrated light (laser) is passed over your skin to disable the hair follicles and prevent hair from growing. With laser, there is permanent hair reduction and in some cases permanent removal. Lasers work best for those with fair skin and dark hair. Individual sessions can last from a few minutes to a few hours, depending on the size of the area being treated. Hair on the upper lip and particularly on the chin may need many treatments as they are in very hormone sensitive parts of the skin. However, a treatment for the upper lip takes only about a minute. After treatment, some people experience long periods without hair re-growth, while others may need occasional touch-ups to remain hair-free. In between treatments, the hair is trimmed or shaved as the melanin target, which is the hair root, has to be present for the laser light to be absorbed. Laser therapy can be uncomfortable, it may cause redness and swelling and can, in rare cases, cause burns or colour changes in your skin. This can be minimized by not treating the skin if it is tanned. While the cost of laser treatment can be high, it may in many instances be more cost-effective due to the longer-term benefits. The most important thing is that the correct laser is used in the right situation and at the appropriate power setting. Make sure to do your research and select a facility with a great reputation and experienced staff.
Prescription Therapy
Two classes of prescription therapies, used to treat hormonal issues, are also used to help manage Unwanted Facial Hair (UFH). The first are hormone blockers, which are drugs that inhibit androgens (male hormones) from working on hair growth. The second are growth inhibitors, which are drugs that block enzymes in the hair itself to inhibit growth.
Hormone Blockers
- Oral contraceptives. Birth control pills, or other hormonal contraceptives, containing the hormones estrogen and progestin, treat UFH by inhibiting androgen production by your ovaries. Oral contraceptives are a common treatment for UFH in women who don't want to become pregnant. Possible side effects include dizziness, nausea, headache, and stomach upset.
- Anti-androgens. These types of drugs block androgens from attaching to their receptors in your body. The most commonly used anti-androgen for treating UFH is spironolactone. Anti-androgens usually take at least three to six months to work. They can decrease the amount of new hair growth, but they are less likely to change the amount of hair you already have. Possible side effects include drowsiness, nausea, irregular menstrual periods, electrolyte disturbances and diarrhea. Because these drugs can cause birth defects, it's important to use good contraception while taking them. Do not take this drug if you think you are or may become pregnant.
- Anti-diabetic. Metformin, a drug normally used in the treatment of diabetes, has in recent years shown to be beneficial in women with polycystic ovarian syndrome, a key cause of UFH.
Growth Inhibitors
- Eflornithine hydrochloride. A topical cream which is applied to the skin, called eflornithine hydrochloride, is the first topical prescription medication that has been approved by Health Canada specifically for slowing the growth of UFH in women. It is indicated for use along with other hair removal techniques. Eflornithine hydrochloride is not a depilatory and does not permanently remove hair or "cure" UFH. What it does is reduce or slow down the hair growth to improve the condition. It is applied twice a day to the area to be treated and, when combined with other hair removal techniques, such as the ones described above, enhances the overall effectiveness of other treatment types.
Coping and Support
It should come as no surprise to the many women affected by excessive facial hair growth that the unwanted hair is only one part of the challenge. Dealing with Unwanted Facial Hair (UFH) can involve much more than simply the efforts to remove the hair. UFH can be emotionally distressing for some women. In fact, in a recent survey, the vast majority of UFH sufferers surveyed (91%) agreed that UFH can have a negative effect on someone's quality of life. Many women with UFH feel extremely self-conscious about having UFH and are even uncomfortable discussing it with others including their own family doctor or other healthcare professional.
Your dermatologist and family physician will appreciate if you are open and honest about how you feel, not only physically, but emotionally, socially and psychologically. He or she will be able to confirm what you have is a common condition and that you are not alone. Most importantly, they will be able to help you to understand that your feelings are in fact valid. Studies report the anxiety and depression associated with excessive facial hair can affect quality of life in much the same way as a diagnosis of gynecological or breast cancer. Taking steps to treat UFH has been shown to help restore confidence and contribute to the overall well-being of those who are affected by it. Speak up: take charge of your overall health by addressing the issues, like UFH, that affect your day-to-day happiness. You are your best health advocate.
Preparing a list of questions will help you make the most of your time with your doctor. For Unwanted Facial Hair (UFH), some basic questions to ask your doctor include:
- What is likely causing my symptoms or condition?
- What are other possible causes?
- Is it normal that my UFH is impacting my self-confidence and overall happiness?
- What kinds of diagnostic tests do I need?
- What are my treatment options?
- If the first treatment I try isn't effective, what will we try next?
- How much will treatment improve my physical signs and symptoms?
- Will I need to be treated long term?
- What are the possible side effects of the medications you're recommending?
- Will the medications you're recommending affect my ability to have children?
- How will you monitor my response to treatment over time?
- Are there alternatives to the primary approach you're suggesting?
- I have these other health conditions. How can I best manage them together?
- Are there any restrictions I need to follow?
- Should I see a specialist?
- Are there brochures or other printed material that I can take home with me? What websites do you recommend?
Don't hesitate to ask your doctor any other questions you have about your condition.
Vitiligo
Overview: What is vitiligo?
The information in this section has been gathered from existing peer-reviewed and other literature and has been reviewed by expert dermatologists on the CSPA Medical Advisory Board.
Vitiligo is a skin condition in which the skin loses melanocytes, the cells that produce melanin, the pigment responsible for skin, hair and eye colour. As a result, irregularly shaped, smooth white patches appear on different parts of the body, sometimes including the inside of the mouth and nose and the retina of the eye. Hair growing on affected areas may also become white because the melanocytes are sometimes lost from the follicles.
In some people with vitiligo, only one or two patches may be present; in others, patches can appear over a large part of the body. It is most noticeable in people with dark skin. There is no way of telling how much pigment loss will occur in any one person. Usually, the disorder is progressive, meaning that over time the white patches will spread to other areas of the body. Spreading can occur slowly or rapidly.
Vitiligo is neither dangerous nor contagious. The condition seems to run in families and occurs more often among people who have certain autoimmune diseases, such as hyper- or hypo-thyroidism (an over- or under-active thyroid gland), adrenocortical insufficiency (underproduction of the corticosteroid hormone by the adrenal gland), rheumatoid arthritis, type 1 diabetes, psoriasis, systemic lupus erythematosus, and pernicious anemia (subnormal red blood cell level caused by an inability to absorb vitamin B12). This suggests that these different autoimmune diseases probably share at least some predisposing genetic or environmental causal factors, although these mostly remain unknown.
Looking Deeper
Many scientists believe that vitiligo is an autoimmune disease where the body’s immune system destroys or disables the melanocytes due to proteins called cytokines. The exact mechanism is not well understood at this point, but may be related to multiple genes plus exposure to environmental risk factors or triggers. Phenols and stress, whether emotional or physical, are suspected to be environmental triggers, but research continues into these and other possibilities.
Fast Facts
- About 0.5 to 1 per cent of the general population has vitiligo.
- The disorder affects both sexes and all races, but is more noticeable in people with darker skin.
- Vitiligo can start at any age, but about half of those with vitiligo develop it before the age of 20, and about 95 per cent before age 40.
- Approximately 20 per cent of vitiligo patients have a family member with the same condition.
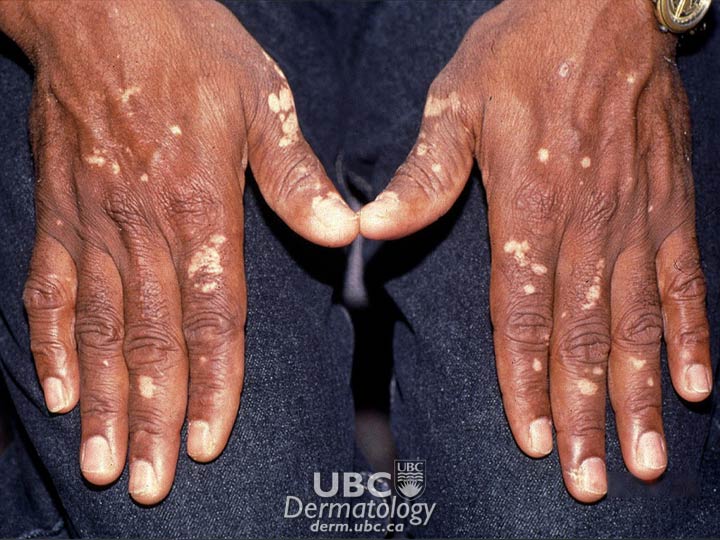 vitiligo-1
vitiligo-1  vitiligo-2
vitiligo-2  vitiligo-3
vitiligo-3
Symptoms
The symptoms of vitiligo include:
- Milky-white, irregularly-shaped patches on the skin
- May first become noticeable on sun-exposed areas (face, hands, feet, arms, legs)
- Other common areas for patches include the armpit, groin, around the mouth, eyes, nostrils, navel, genital and rectal areas
- Premature whitening or greying of hair on scalp, eyelashes, eyebrows or beard
- Colour loss in the mucous membranes inside the mouth and nose (less common)
Vitiligo generally appears in one of three patterns:
- Generalized pattern (most common): patches are spread all over the body, often symmetrically
- Focal pattern: depigmented patches are limited to one or a few areas
- Segmental pattern: colour loss occurs in patches on only one side of the body
Looking Deeper
Diagnosis and Treatment
Diagnosis is by physical examination, medical history, and laboratory tests.
Physical Exam
A doctor will confirm the presence of white patches on the skin in expected areas in one of the three typical patterns. A Woods’ Lamp, which shines ultraviolet light onto the skin, is frequently used to examine areas, as vitiligo glows under this type of light.
Medical History
Your family doctor will ask you if you:
- or any family member have an autoimmune disease
- have had a rash, sunburn, or other skin problem before the appearance of the white patches
- have suffered recent stress or illness
- have greyed before the age of 35
- are sensitive to the sun
Laboratory Tests
Your doctor may occasionally need to take a skin sample, but most cases of vitiligo can be diagnosed by direct visual examination. Skin affected by vitiligo shows no pigment-producing melanocytes. Blood tests may also be done to rule out pernicious anemia, thyroid disease or another autoimmune disease.
Treatment
Vitiligo cannot be cured, but treatments are available that might even out skin colour. Fair-skinned patients with a few small patches may choose not to treat vitiligo, and sunscreen and cosmetics may be all that is needed to camouflage the patches. Vitiligo can be disguised with a variety of make-up or a homemade stain made from food colouring and rubbing alcohol, although commercially available products give a more natural skin colour match.
Children can be treated with topical steroids, topical immunomodulators, or narrowband ultraviolet B (UVB) light treatment; they frequently repigment faster than adults, so catching it early can make it easier to treat before patches become larger and more numerous.
Patients with darker skin or those with patches that are large or great in number may opt for medical treatment to either restore white patches to their original colour (repigment) or destroy remaining colour to match the white patches (depigment). Some commonly used treatments are described below.
Topical Corticosteroid Therapy
Corticosteroid creams can return colour to the skin, particularly if applied at an early stage. A mild topical cream or ointment may be prescribed for young children (under 10 years) while adults use a stronger form. Treatment is simple—the cream or ointment is applied to the white patches—but monitoring must be conducted for side effects such as skin thinning or streaking. Corticosteroids may be used along with a topical vitamin D derivative. Results may be seen after three months but are not as effective as psoralen photochemotherapy (see below).
Topical Immunomodulator Therapy
A relatively new treatment for vitiligo uses topical immunomodulators, such as tacrolimus and pimecrolimus, which work to regulate the local immune system activities that result in depigmentation. They are now commonly prescribed by dermatologists for facial and other areas and can be used for longer periods without the side effects of corticosteroids. Side effects include transient burning and stinging sensations in the skin and a potential increased risk for cancer, although this is considered extremely rare.
Narrow-band Ultraviolet B (NB-UVB) Therapy
Narrow-band UVB therapy is an alternative to UVA therapies. Narrow-band UVB light is administered up to three times a week without pre-application of psoralen. This treatment is simpler and may be safer than previous forms of ultraviolet therapies. Studies have shown that it is now considered the treatment of choice for vitiligo covering more than 10-20 per cent of the body.
Depigmentation
Depigmentation involves fading normal skin to match the already white areas, an option that may be considered if vitiligo affects more than 50 per cent of the body. Monobenzylether of hydroquinone (monobenzone) is applied twice daily to pigmented areas until they match depigmented areas. However, there are a number of adverse effects. Major side effects include redness and swelling of the skin and permanent sun sensitivity. Other side effects are itching, dry skin, and abnormal darkening of the membrane covering the whites of the eyes. Depigmentation is permanent and irreversible and patients need to think carefully before pursuing this option.
Transplant Surgery
Only a small percentage of patients are eligible for vitiligo skin transplant surgery. Three options for surgical treatment are available:
- “Minipunch” skin transfer: This method uses the person’s own tissue to treat small patches. Small pieces of normal skin are removed and attached to depigmented sites. Possible complications include infection at donor or recipient sites (rare), scarring, a cobblestone skin texture, spotty pigmentation, and vitiligo appearing at the donor site due to skin trauma.
- Blister grafting: This process uses heat, cold or suction to produce blisters over pigmented and depigmented skin. The tops of the pigmented blisters are removed and transplanted to the depigmented skin areas. The risks are scarring and a cobblestone appearance.
- Autologous melanocyte transplant: In this procedure, a sample of normal pigmented skin is isolated in a laboratory dish containing a special cell suspension solution. Once enough melanocytes have been isolated, they are transplanted to depigmented areas of the skin.
Tattooing (micropigmentation)
In this method, pigment is inserted into the skin. It has proven to be most effective in the lip area in dark-skinned people. Disadvantages are that it is difficult to match natural skin colour and any tattooing can fade with time. A possible side effect in the lip area is that it may lead to blisters caused by the herpes simplex virus in people already infected with the virus. Side effects in other areas are that it may cause vitiligo to spread in the tattooed area due to skin trauma. Finally, tattooing is not reversible, since tattoos used for micropigmentation cannot be safely removed by laser technology. Generally, this treatment is not recommended in most cases.
Research on vitiligo is ongoing and includes a number of studies exploring the role of skin trauma as well as the identification and analysis of genes that may cause or contribute to the condition. Researchers may be testing new medications for vitiligo as part of these research studies.
*All information on medical treatments on this site is provided as an overview only. For a complete and up-to-date list of side effects, warnings and precautions, read the product’s package insert and consult your doctor or a pharmacist.
**If you are considering an alternative or complementary therapy, discuss it with your doctor first, and always be sure to keep your doctor up to date about any vitamins, supplements, or other forms of alternative treatment you are taking. Like any medication, alternative therapies can interact with other medications/treatments and, in some cases, have side effects of their own. Remember that “natural” does not necessarily mean “safe.”
Coping and Support
Vitiligo does not impact a person’s overall physical health. However, if the white patches are in a prominent place (e.g., hands or face), you may be self-conscious and experience embarrassment, depression or anxiety. In these situations, psychological counselling can restore your self-confidence and positive self-image.
Vitiligo support groups can also be a useful forum for sharing concerns and coping strategies. Associations such as Vitiligo Support International can provide additional information.
The physical side of vitiligo can also be managed. For example, sun sensitivity can be controlled through the use of sunscreen and reducing exposure to the sun. This further minimizes tanning so that the contrast between normal and depigmented skin becomes less noticeable. And cosmetics, such as make-up, self-tanning lotions and dyes can effectively cover depigmented patches.
Warts
Overview: What is warts?
The CPSA gratefully acknowledges Jessica Ho, MSc Public Health, MD candidate, Queen’s University, and Yuka Asai, MD, PhD for assistance in the preparation of this report. August 2021.
Warts are small growths on the skin caused by the human papillomavirus (HPV). This virus invades skin cells and enters a resting period, called latency, that may last for months or years. During latency, the virus multiplies and invades additional cells, which then take on the appearance of warts. Over 200 strains of HPV have been identified from DNA sequence data,1 more information on HPV can be found here (link to HPV section). Certain strains tend to infect specific areas of the skin and there are six primary types of warts.
Primary types of warts:
- Common
- Filiform (warts that have long, narrow strands that extend about 1 to 2 millimeters from the skin)
- Flat
- Plantar
- Periungual (located around a nail)
- Genital
Warts are contagious and can spread through direct and indirect contact. This includes direct spread via skin to skin contact as well as indirectly from surfaces (fomites). All warts are more likely to spread by trauma to the skin which may occur through nail-biting, picking of the wart, rubbing (such as via callouses) and activities like shaving. Genital warts may be spread through skin to skin contact that occurs with sexual activity. Fomites are objects or surfaces that can spread infections like HPV. Spread via fomites may occur on contact with surfaces such as shower stall floors, swimming pool decks and improperly cleaned instruments that have been in contact with an HPV infection. Oral warts may also occur and can be seen in uncommon conditions such as focal epithelial hyperplasia (Heck’s disease).
Some people may have a predisposition to HPV infection and the development of warts. Often these are people who have immunodeficiencies where the body is more susceptible to infections such as HPV. While these are rare, immunodeficiencies include conditions like epidermodysplasia verruciformis (EDV).
Although warts frequently recur after treatment, many will disappear spontaneously within two to three years. Some strains of HPV that cause genital warts have the potential to cause cancer of the cervix, vulva, penis and anus. More information about the development of cancer related to HPV infections can be found in the HPV section (link to HPV section).
Fast Facts
Non-genital warts:
- Approximately 7 to 12 percent of the general population is affected by warts.
- Both men and women are equally affected by warts. Up to 50 percent of all men and women have been infected by HPV at some point in their lives.
- Warts are common in children. Approximately 10 to 20 percent of school-aged children are affected.
- In children, the incidence of warts peaks at 12 to 16 years of age.
- Warts are twice as frequent in those that identify as White compared to those of African or Asian descent.
- Approximately 65 percent of non-genital warts disappear without treatment within two to three years.
Genital warts:
- Genital warts are considered the most common sexually transmitted disease, affecting approximately 1 percent of the population.
- Genital warts are most common in individuals aged 17 to 33 years of age.
- It is estimated that 75 percent of sexually active men and women will experience at least one genital HPV infection in their life.
Symptoms
The symptoms of warts vary depending on their location on the body.

Common Warts (hands/knees)
- Skin-coloured lumps of 1 mm to over 10 mm in diameter with a rough, irregular surface

Filiform Warts (nose/mouth/beard area)
- Skin-coloured bumps with growths that look like threads sticking out of them
Flat Warts (face/hands/shins/knees)
- Fairly smooth individual bumps of 1 mm to 5 mm in diameter
- Can form groups of hundreds of bumps
- Can spread rapidly as a result of everyday activities, such as shaving

Plantar Warts (sole of foot)
- Thick, scaly lesions or rough, spongy lesions with tiny dark spots inside
- Smooth, brown or yellow-grey surface that is often flattened
- On areas of pressure, such as the heel or ball
- Can fuse together to form larger mosaic warts
- Occasionally accompanied by foot pain

Periungual Warts (nails)
- Rough bumps with an uneven surface and border
- Under and around toenails and fingernails
- Can affect nail growth
Genital Warts
- Soft, moist, flesh-coloured bumps
- On the vagina (inside and outside), cervix or anus in women; on the tip or shaft of the penis, on the scrotum or around the anus in men
- Symptoms are often absent, but the condition is still contagious and can lead to complications
Diagnosis and Treatment
Only a physician can confirm whether or not you have warts, so if you experience any wart-related signs or symptoms, visit your doctor. Some skin growths that may resemble warts are actually moles, corns, calluses, skin tags, or even skin cancer. It is particularly important to seek help if you suspect that you have genital warts because they are sometimes linked to the development of cancer. More information relating to genital warts related to cancer can be found here.
Your physician will perform a physical examination that consists of a visual inspection, sometimes with a special magnifying instrument called a dermatoscope. Occasionally, a biopsy of the lesion will be performed if the physician is uncertain of the diagnosis. It is recommended that individuals with anogenital warts be screened for other sexually transmitted infections (STIs), and women should be referred for gynecologic screening. Women with genital warts may undergo a Pap test to make sure they have no signs of cervical cancer as these are often asymptomatic in early stages.
Although warts can sometimes disappear without treatment, many people choose to treat their warts if they are unsightly, start to spread, or cause discomfort. Talk to your doctor about whether treatment is appropriate and which treatment may be right for you.
Lifestyle Changes and Skin-care Strategies
Non-genital Warts
If you develop warts, you can make several lifestyle changes to help them heal properly and prevent them from spreading:
|
AVOID |
INSTEAD |
|
|
Genital Warts
You can change your lifestyle to prevent the spread of genital warts once they occur:
|
AVOID |
INSTEAD |
|
|
Medical Treatments
Most wart treatments are topical. Some treatments can be carried out at home, and some must be applied by a doctor. They each use a different chemical to achieve the same thing; to kill the wart cells, causing them to peel and fall off. Treatments are also available to help your body’s immune system attack the wart cells. The type of wart treatment you will use depends on what type of warts you have. If you are currently using steroids, have a condition that impairs your circulation or puts you at risk for neuropathies (such as diabetes); check with a doctor before initiating any of these treatments.
Topical Treatments
Cantharidin and cantharidin combination products cause skin to blister and peel off. They are used by doctors for the treatment of warts and molluscum.2 They work by causing the formation of blisters within 24 to 48 hours and healing usually occurs within 4 to 7 days of application.2 Complications are rare when cantharidin is used appropriately, though there may be mild to moderate pain, temporary redness, a temporary burning sensation or itchiness of the skin with application. These products are available alone and in combination with other wart-removing agents such as salicylic acid and podophyllin.
Imiquimod is a prescription immune-response modifier that causes your body’s normal immune defences to work against the wart. It is provided as a prescription cream and can be used to treat external genital warts (i.e., warts on the penis or the vulva), and warts near the anus. It is also used for other kinds of skin conditions such as cancerous and pre-cancerous skin growths. For genital and perianal warts, imiquimod is usually applied at bedtime and used three times per week for up to 16 weeks, while other formulations of it are applied every night until clear. You should not apply a bandage over the cream, but you may apply a cotton gauze pad to the area. Some people experience long-term changes in skin colour such as lightening or darkening, in the treated area. If you experience serious irritation following treatment, you can discontinue imiquimod for a few days and then resume treatment when the reaction subsides. Most people experience some inflammation, reddening and irritation in the treated area. Uncommonly, some women have difficulty urinating as a result of the inflammation or develop a flu-like reaction (including fever, tiredness, muscle aches).
Liquid nitrogen (cryotherapy) is one of the most common treatments for warts. Liquid nitrogen at very low temperatures is used to “freeze off” or “freeze burn” the wart, causing the cells in the wart to die and the wart to peel off. Liquid nitrogen is extremely dangerous to handle, and therefore it must only be applied by a doctor. You may require regular repeated treatments to remove the wart completely, and occasionally treatment may cause some scarring after the wart is removed.
Podophyllin and podofilox (podophyllotoxin) cause skin cells, including the wart cells, to die and then peel off. These preparations are used by doctors to remove external genital warts, common warts and plantar warts. Podophyllin is available alone and in combination with other wart-removing agents (salicylic acid and cantharidin). Your doctor will apply the first dose of podophyllin and will instruct you on how to apply the later doses, usually once or twice a day for up to three days, followed by at least four days of no treatment. On the advice of your doctor, you may repeat this course of treatment (three days of treatment followed by four days of no treatment) for up to four weeks. When using podophyllin, apply it directly to the warts, using a layer of petroleum jelly to protect the surrounding skin. It will dry to form a film surrounding the wart. You should not use podophyllin if you are pregnant.
Salicylic acid is one of several strong acids used to “burn off” warts. In general, removal of the external thick dead skin (keratin layer) will improve the efficacy of medical therapies applied to the skin. To use, first soak the affected area in warm water for five minutes and remove softened wart tissue with a washcloth or emery board. Apply the gel directly to the wart and allow it to dry and form a barrier around the wart. Treat once a day until the wart is cleared; if you develop any discomfort, take a break from treatment, and then restart as needed. This product and other strong acids must not be used near the eyes or mucous membranes. In addition, salicylic acid is flammable and should be kept tightly capped and away from heat sources or open flames.
Other strong acids (bichloroacetic acid/trichloroacetic acid) can be used to spot-treat warts. Bichloroacetic acid and trichloroacetic acid are used for several kinds of warts, including genital and plantar warts. To avoid the risk of any damage to your skin, these treatments must be applied by your doctor. You may require repeated treatments to remove the wart completely.
Other Treatments
Some medications that are officially approved for treating other conditions and diseases have been tried in the treatment of warts with variable success. Some alternative treatments and home remedies have also been studied in the treatment of warts, but the evidence is either mixed or limited. These treatments are included here for information only.
- Prescription:Cimetidine, intralesional immunotherapy (e.g., interferon, bleomycin), 5-fluorouracil, epinephrine
- Other:Laser therapy, aminolevulinic acid with photodynamic therapy infrared coagulation, duct tape coverage, surgical therapies (e.g., surgical excision)
Footnotes:
**If you are considering an alternative or complementary therapy, discuss it with your doctor first, and always be sure to keep your doctor up to date about any vitamins, supplements, or other forms of alternative treatment you are taking. Like any medication, alternative therapies can interact with other medications/treatments and, in some cases, have side effects of their own. Remember that “natural” does not necessarily mean “safe.”
Coping and Support
Non-genital warts don’t usually have a major impact on patients’ health though large or multiple warts may be unsightly and may affect quality of life. Aside from the pain caused by plantar warts, non-genital warts pose no risk or discomfort to otherwise healthy individuals. However, seeking medical treatment for warts may resolve any discomfort and improve the cosmesis of the skin.
Management of genital warts involves the modification of sexual habits to prevent the spread to sexual partners. Ensuring safe sexual practices will reduce the risk of transmission to others. Preventing the development of genital warts through vaccination against HPV will also reduce the risk of genital warts that can lead to cancer. More information on the prevention of HPV can be found in the section on HPV. If you are having trouble coping with your condition, it is important to see additional support through your physician, or other mental health supports as appropriate.
Resources
If you are living with warts or know someone who is, you may want to stay up-to-date on the condition as well as current treatments and news.
Other Resources
coming soon
Wounds
Overview: What are chronic wounds/ulcers?
The information in this section has been gathered from existing peer-reviewed and other literature and has been reviewed by expert dermatologists on the CSPA Medical Advisory Board.
Chronic wounds/ulcers are open areas of the skin that do not heal despite weeks of careful treatment. And even when these wounds are successfully treated, they tend to recur.
Acute wounds typically heal in one to three weeks in a dynamic process that restores the integrity and function of the skin and the underlying tissue. If a wound does not heal in four to 12 weeks, it is considered chronic. With any wound, natural healing occurs in clearly defined stages, but chronic wounds get stuck at one of the stages and cannot get past it.
Causes
Chronic wounds and ulcers are caused by poor circulation, either through cardiovascular issues or external pressure from a bed or wheelchair. People affected by chronic wounds are typically sedentary, often bedridden, wheelchair-bound and/or have diabetes. Good circulation requires regular bodily movement such as going for a walk. Chronic wound types include:
- Pressure ulcers (also known as bed sores)
- Diabetic foot ulcers
- Leg ulcers (venous stasis and arterial ulcers)
- Ulcers resulting from blood disorders
 skin ulcer 1
skin ulcer 1
Symptoms
A chronic wound is a wound that does not progress toward closure in a timely manner. The typical signs of a chronic wound include:
- Pain (except in many cases of diabetic foot ulcer, where there is no sensation at all)
- Erythema (inflammation or redness of the skin)
- Edema (swelling)
- Heat
- Purulence (the presence of pus)
Diagnosis and Treatment
If you suspect you have a chronic wound or a developing ulcer, seek medical care immediately, particularly if you have any of the following conditions:
- Diabetes
- Arterial disease
- Chronic edema (swelling) of the lower extremities
- A family history of collagen vascular disease, such as scleroderma or rheumatoid arthritis
In addition, a slow-healing wound may indicate an infection or other significant problem that is affecting the whole body.
Treatment for chronic wounds take time. The goals of treatment are usually to:
- Keep the wound infection-free
- Absorb any excess discharge
- Keep the wound clear of dead tissue, usually through debridement (removal of tissue)
- Maintain a moist wound environment
- Supply compression to control the edema (swelling) in the case of venous stasis ulcers
- Manage pain
- Offload pressure from the affected area (for diabetic foot and pressure ulcers)
- Promote more activity to increase circulation
- Manage the person’s medical issues
Your doctor will prescribe the course of therapy that is best for your type of wound.
Other steps you can take to promote healing include:
- Ensuring you eat an adequate, well-balanced diet
- Losing weight if necessary
- Stopping smoking (smoking impairs circulation)
*All information on medical treatments on this site is provided as an overview only. For a complete and up-to-date list of side effects, warnings and precautions, read the product’s package insert and consult your doctor or a pharmacist.
**If you are considering an alternative or complementary therapy, discuss it with your doctor first, and always be sure to keep your doctor up to date about any vitamins, supplements, or other forms of alternative treatment you are taking. Like any medication, alternative therapies can interact with other medications/treatments and, in some cases, have side effects of their own. Remember that “natural” does not necessarily mean “safe.”
Coping and Support
People living with chronic wounds typically have other medical conditions that affect their everyday life. Congestive heart failure and diabetes are just two examples, as are any diseases that may keep them bedridden or wheelchair-bound. People with ulcers and chronic wounds can face many challenges, including:
- Pain
- Altered or limited mobility
- Sleep disorders
- Difficulties maintaining body hygiene
- Depression
- Low self-esteem
- Feelings of frustration
- Social isolation
For these reasons, a chronic wound or ulcer can be psychologically stressful for a person as well as for their families, friends and caregivers. For the person with the condition, they may have thoughts and feelings about:
- Having a low level of control over their condition
- Being unable to predict how long and how severe their wound will be
- Seeing the wound as proof that things are getting worse or that they are “falling apart”
- Having few outlets for their frustration
- Not having enough social support
In spite of these challenges, many people do adjust to living with a chronic wound. Those people who do best tend to do one or all of the following:
- Cope by comparison—that is, they emphasize the positive aspects of their own lives compared with those less fortunate
- Focus on feeling healthy in spite of the wound
- View the condition as part of the ageing process and adjust their expectations accordingly
- Simply be positive
If you have a chronic wound or are at risk for a chronic wound, you can help yourself by doing the following:
Venous leg ulcer:
- Wear your stockings every day
- Exercise regularly. Walking is all it takes, as compression bandages and stockings work best when you move. If you are less mobile, exercise your leg muscles by moving your foot up and down at the ankle
- When you sit, keep your legs raised by putting your feet on a stool or chair
Diabetic foot ulcer:
- Check your feet regularly for small cuts and sores. These can grow into large wounds. Use a mirror or ask your partner to help if you can’t see the bottoms of your feet
- If you already have a wound on your foot, see your doctor about special footwear to take the pressure off the spot. Don’t continue to walk on the wound, even if you can’t feel pain
Pressure ulcer:
- Remove the source of pressure from the affected area. If you lack the mobility or strength to do so, have someone help you adjust your position frequently
All types:
- If you smoke, stop
- Eat a healthy, balanced diet. If you’re overweight, do what you can to lose weight
- Ask your doctor for a referral to a wound-care specialist
People with chronic wounds or leg ulcers can find additional support online. The Canadian Association of Wound Care has information and resources that can help.









